August Gilbert P, Caprio Sonia, Fennoy Ilene, Freemark Michael, Kaufman Francine R, Lustig Robert H, Silverstein Janet H, Speiser Phyllis W, Styne Dennis M, Montori Victor M
George Washington University School of Medicine, Washington, D.C. 20037, USA.
J Clin Endocrinol Metab. 2008 Dec;93(12):4576-99. doi: 10.1210/jc.2007-2458. Epub 2008 Sep 9.
Our objective was to formulate practice guidelines for the treatment and prevention of pediatric obesity.
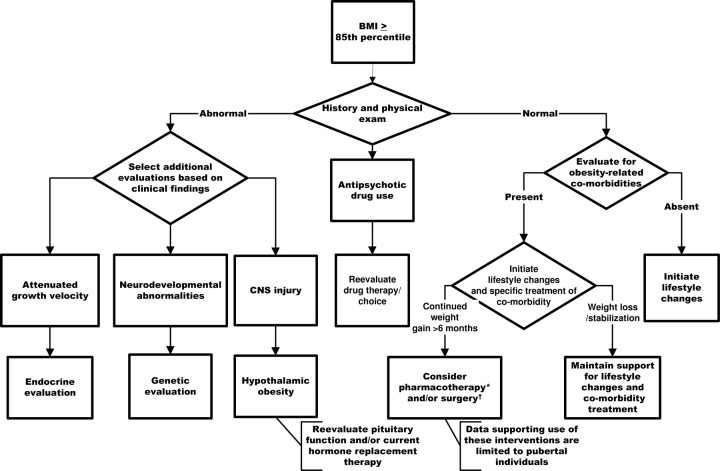
We recommend defining overweight as body mass index (BMI) in at least the 85th percentile but < the 95th percentile and obesity as BMI in at least the 95th percentile against routine endocrine studies unless the height velocity is attenuated or inappropriate for the family background or stage of puberty; referring patients to a geneticist if there is evidence of a genetic syndrome; evaluating for obesity-associated comorbidities in children with BMI in at least the 85th percentile; and prescribing and supporting intensive lifestyle (dietary, physical activity, and behavioral) modification as the prerequisite for any treatment. We suggest that pharmacotherapy (in combination with lifestyle modification) be considered in: 1) obese children only after failure of a formal program of intensive lifestyle modification; and 2) overweight children only if severe comorbidities persist despite intensive lifestyle modification, particularly in children with a strong family history of type 2 diabetes or premature cardiovascular disease. Pharmacotherapy should be provided only by clinicians who are experienced in the use of antiobesity agents and aware of the potential for adverse reactions. We suggest bariatric surgery for adolescents with BMI above 50 kg/m(2), or BMI above 40 kg/m(2) with severe comorbidities in whom lifestyle modifications and/or pharmacotherapy have failed. Candidates for surgery and their families must be psychologically stable and capable of adhering to lifestyle modifications. Access to experienced surgeons and sophisticated multidisciplinary teams who assess the benefits and risks of surgery is obligatory. We emphasize the prevention of obesity by recommending breast-feeding of infants for at least 6 months and advocating that schools provide for 60 min of moderate to vigorous daily exercise in all grades. We suggest that clinicians educate children and parents through anticipatory guidance about healthy dietary and activity habits, and we advocate for restricting the availability of unhealthy food choices in schools, policies to ban advertising unhealthy food choices to children, and community redesign to maximize opportunities for safe walking and bike riding to school, athletic activities, and neighborhood shopping.
我们的目的是制定儿童肥胖治疗与预防的实践指南。
我们建议将超重定义为体重指数(BMI)至少处于第85百分位数但低于第95百分位数,将肥胖定义为BMI至少处于第95百分位数,常规情况下无需进行内分泌检查,除非身高增长速度减缓或与家族背景或青春期阶段不相符;如果有遗传综合征的证据,将患者转诊给遗传学家;对BMI至少处于第85百分位数的儿童评估肥胖相关合并症;并将规定和支持强化生活方式(饮食、体育活动和行为)改变作为任何治疗的前提条件。我们建议在以下情况考虑药物治疗(结合生活方式改变):1)仅在强化生活方式改变的正规计划失败后的肥胖儿童中;2)仅在尽管进行了强化生活方式改变但严重合并症仍然存在的超重儿童中,特别是在有2型糖尿病或心血管疾病家族史的儿童中。药物治疗应由有使用抗肥胖药物经验并了解不良反应可能性的临床医生提供。我们建议对BMI高于50kg/m²或BMI高于40kg/m²且有严重合并症且生活方式改变和/或药物治疗失败的青少年进行减肥手术。手术候选者及其家人必须心理稳定且能够坚持生活方式改变。必须能够获得评估手术利弊的经验丰富的外科医生和复杂的多学科团队。我们强调通过建议婴儿至少母乳喂养6个月以及倡导学校在所有年级每天提供60分钟的中度至剧烈运动来预防肥胖。我们建议临床医生通过关于健康饮食和活动习惯的预期指导来教育儿童和家长,我们倡导限制学校提供不健康食品选择,制定禁止向儿童宣传不健康食品选择的政策,以及进行社区重新设计以最大限度增加安全步行和骑自行车上学、体育活动及邻里购物的机会。