Sarrassat Sophie, Senghor Paul, Le Hesran Jean Yves
Unité de Recherche, Santé de la mère et de l'enfant en milieu tropical, IRD, UR010, Université Pairs Descartes, Faculté de Pharmacie, Paris, France.
Malar J. 2008 Oct 24;7:215. doi: 10.1186/1475-2875-7-215.
In Thailand, South Africa and Zanzibar, a decrease in malaria morbidity was observed following the introduction of artemisinin-based combination therapy (ACT). In Senegal, therapeutic trials supervised the in vivo efficacy of artesunate plus amodiaquine from 1999 to 2005 at the M'lomp village dispensary. The trends in malaria morbidity in this village were evaluated from 2000 to 2002.
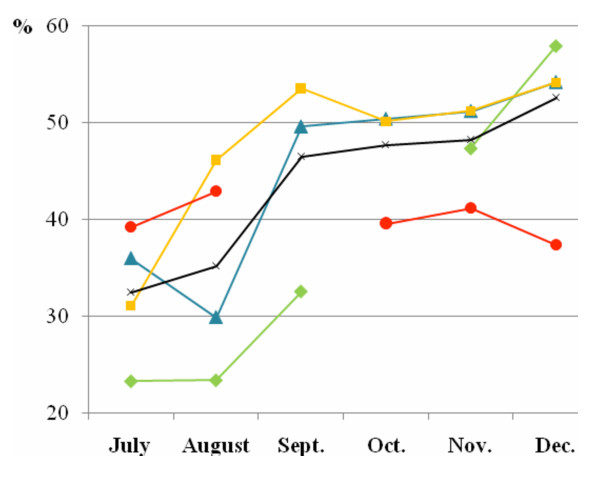
Each year, between July and December inclusive, fevers treated with antimalarials and slide-proven, uncomplicated malaria cases were collected from dispensary health records. Data were also collected in 1998, just prior to ACT introduction. Pearson's chi square tests and Student tests were used to compare two percentages or two means respectively (alpha = 0.05).
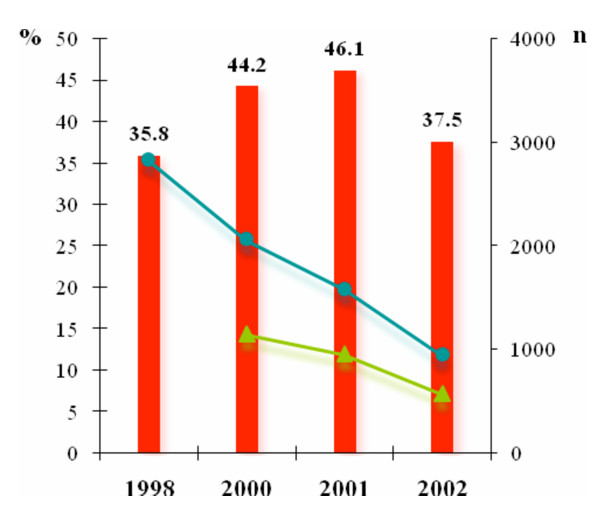
Between 1998 and 2002, the total number of fevers treated with antimalarials and their repetitiveness progressively decreased: From 2824 to 945 fevers and from 17.6% to 9.7% (RR1998-2002 = 0.55; [0.44-0.69]; p < 0.0001) respectively. Considering uncomplicated malaria cases only, a decrease was observed in their total number between 2001 and 2002, from 953 to 570 cases. The incidence rate and repetitiveness also decreased. The incidence rate fell from 46.1% in 2001 to 37.5% in 2002 (p < 0.0001) and the repetitiveness decreased from 13.0% in 2000 to 6.6% in 2002 (RR2000-2002 = 0.51; [0.35-0.72]; p = 0.0001).
The percentage of uncomplicated malaria cases treated with ACT increased, from 18.9% in 2000 to 64.0% in 2002, making it tempting to conclude an impact on malaria morbidity. Nonetheless, the decline in incidence rate of uncomplicated malaria was slight and a lower recorded rainfall was reported in 2002 which could also explain this decline. The context in which ACT is introduced affects the impact on malaria morbidity. In M'lomp, in contrast to studies in Thailand, South Africa and Zanzibar, ACT coverage of malaria cases was low and no vector control measure was deployed. Moreover, the malaria transmission level is higher. In sub-Saharan countries, in order to optimize the impact on malaria morbidity, ACT deployment must be supported, on the one hand, by a strengthening of public health system to ensure a high ACT coverage and, on the other hand, by others measures, such vector control measures.
在泰国、南非和桑给巴尔,采用青蒿素联合疗法(ACT)后,疟疾发病率有所下降。在塞内加尔,1999年至2005年期间在姆隆普村诊所对青蒿琥酯加阿莫地喹的体内疗效进行了治疗试验。对该村庄2000年至2002年期间的疟疾发病趋势进行了评估。
每年7月至12月(含7月和12月),从诊所健康记录中收集接受抗疟治疗的发热病例以及经涂片证实的非复杂性疟疾病例。还在1998年,即ACT引入之前收集了数据。分别使用Pearson卡方检验和学生检验来比较两个百分比或两个均值(α = 0.05)。
1998年至2002年期间,接受抗疟治疗的发热病例总数及其重复性逐渐下降:分别从2824例降至945例,从17.6%降至9.7%(RR1998 - 2002 = 0.55;[0.44 - 0.69];p < 0.0001)。仅考虑非复杂性疟疾病例,2001年至2002年期间其总数有所下降,从953例降至570例。发病率和重复性也有所下降。发病率从2001年的46.1%降至2002年的37.5%(p < 0.0001),重复性从2000年的13.0%降至2002年的6.6%(RR2000 - 2002 = 0.51;[0.35 - 0.72];p = 0.0001)。
接受ACT治疗的非复杂性疟疾病例百分比从2000年的18.9%增至2002年的64.0%,这使得人们很容易得出ACT对疟疾发病率有影响的结论。然而,可以解释这种下降的是,非复杂性疟疾发病率的下降幅度较小,且2002年记录的降雨量较低。引入ACT的背景会影响对疟疾发病率的影响。与泰国、南非和桑给巴尔的研究不同,在姆隆普,ACT对疟疾病例的覆盖率较低,且未采取病媒控制措施。此外,疟疾传播水平较高。在撒哈拉以南国家,为了优化对疟疾发病率的影响,一方面,必须加强公共卫生系统以确保ACT的高覆盖率,另一方面,必须采取其他措施,如病媒控制措施,以支持ACT的推广。