Burton G J, Yung H-W, Cindrova-Davies T, Charnock-Jones D S
Department of Physiology, Development and Neuroscience, University of Cambridge, UK.
Placenta. 2009 Mar;30 Suppl A(Suppl):S43-8. doi: 10.1016/j.placenta.2008.11.003. Epub 2008 Dec 9.
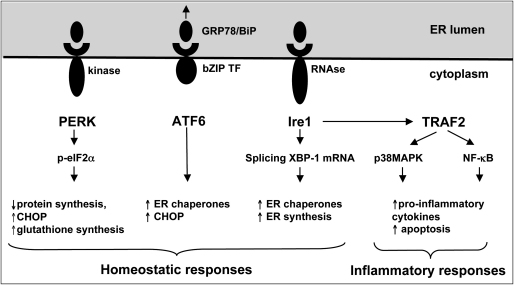
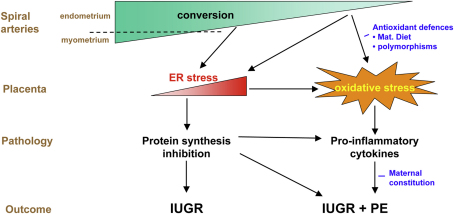
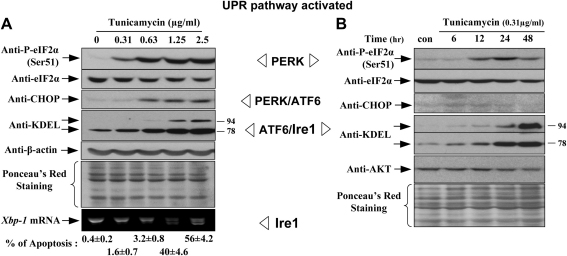
The pregnancy complications of unexplained intrauterine growth restriction and early onset preeclampsia are thought to share a common aetiology in placental malperfusion secondary to deficient maternal spiral artery conversion. A key question is whether the contrasting clinical manifestations reflect different placental pathologies, or whether they are due to altered maternal responses to a common factor derived from the placenta. Recently, molecular evidence of protein synthesis inhibition secondary to endoplasmic reticulum stress has provided an explanation for the small placental phenotype in both conditions. However, other pathways activated by more severe endoplasmic reticulum stress are only observed in placentas from pregnancies associated with early onset preeclampsia. Here, we review the literature and conclude that there is evidence of greater maternal vascular compromise of the placenta in these cases. We speculate that in cases of normotensive intrauterine growth restriction the placental pathology is centred predominantly around endoplasmic reticulum stress, whereas in cases complicated by preeclampsia oxidative stress is further superimposed. This causes the release of a potent mix of pro-inflammatory cytokines, anti-angiogenic factors and trophoblastic aponecrotic debris into the maternal circulation that causes the peripheral syndrome. Maternal and fetal constitutional factors may modulate how the placenta responds to the maternal vascular insult, and how the mother is affected by the placental factors released. However, the principal conclusion is that the difference between these two conditions lies in the severity of the initiating deficit in spiral arterial conversion, and the relative degrees of endoplasmic reticulum stress and oxidative stress induced in the placenta as a result.
不明原因的子宫内生长受限和早发型子痫前期的妊娠并发症被认为在病因上具有共性,即由于母体螺旋动脉转化不足导致胎盘灌注不良。一个关键问题是,这两种截然不同的临床表现是反映了不同的胎盘病理状态,还是由于母体对源自胎盘的共同因素的反应改变所致。最近,内质网应激继发蛋白质合成抑制的分子证据为这两种情况下胎盘小的表型提供了解释。然而,更严重的内质网应激激活的其他途径仅在与早发型子痫前期相关的妊娠胎盘中观察到。在此,我们回顾文献并得出结论,在这些病例中存在胎盘母体血管受损更严重的证据。我们推测,在血压正常的子宫内生长受限病例中,胎盘病理主要围绕内质网应激,而在子痫前期合并病例中,氧化应激进一步叠加。这导致促炎细胞因子、抗血管生成因子和滋养层细胞凋亡碎片的强效混合物释放到母体循环中,从而引发外周综合征。母体和胎儿的体质因素可能会调节胎盘对母体血管损伤的反应方式,以及母亲受胎盘释放因子影响的方式。然而,主要结论是,这两种情况的差异在于螺旋动脉转化起始缺陷的严重程度,以及由此在胎盘中诱导的内质网应激和氧化应激的相对程度。