Department of Anaesthesiology, University Hospital Heidelberg, Heidelberg, Germany.
Crit Care. 2009;13(1):R11. doi: 10.1186/cc7709. Epub 2009 Feb 6.
One of the main causes of death in European and US intensive care units is sepsis. It involves a network of pro-inflammatory cytokines such as TNF-alpha, IL-1beta and IL-6. Furthermore, there is an up regulation of transcription factors such as nuclear factor (NF) kappaB. It has previously been shown that clonidine is able to significantly reduce pro-inflammatory cytokines in surgical patients. We therefore hypothesise that the clinically used central alpha-2 agonist clonidine has the ability to improve survival in experimental sepsis by inhibiting the sympathetic tone and consequently inhibiting the pro-inflammatory cytokine release.
To investigate this therapeutic potential of clonidine in a prospective randomised laboratory investigation we used a murine model of caecal ligation and puncture (CLP) induced sepsis. Animals receiving pre-emptive injections were treated with either clonidine (5 microg/kg) or dexmedetomidine (40 microg/kg) 12 and 1 hours before the operation, as well as 1, 6 and 12 hours afterwards. Another group of animals only received clonidine (5 microg/kg) 1, 6 and 12 hours after the operation, while the pre-emptive injections were normal saline. The control groups received solvent injections at the respective time points.
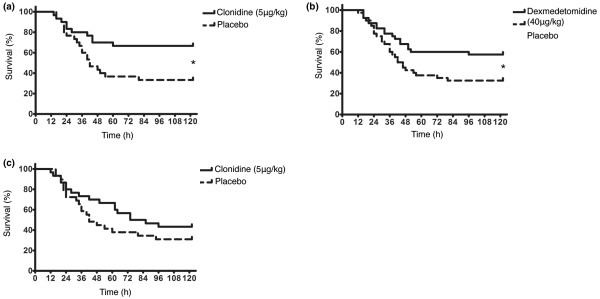
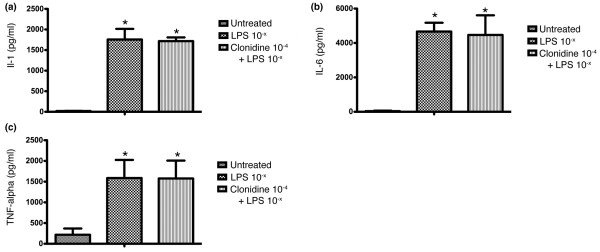
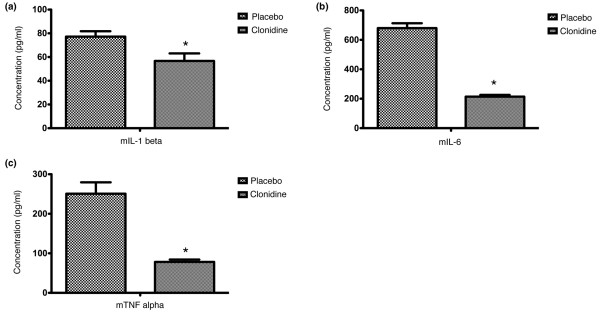
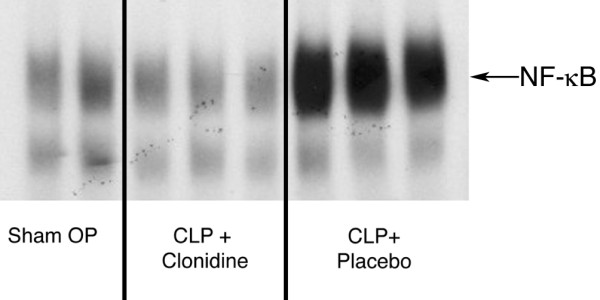
Pre-emptive administration of a central sympatholytic significantly reduced mortality (clonidine: p = 0.015; dexmedetomidine: p = 0.029), although postoperative administration of clonidine failed to significantly prolong survival. Furthermore pre-emptive administration of clonidine significantly attenuated the cytokine response after CLP-induced sepsis (mIL-1beta: p = 0.017; mIL-6: p < 0.0001; mTNF-alpha: p < 0.0001), preserved blood pressure control (p = 0.024) and down-regulated the binding activity of NF-kappaB. There were no changes in the pro-inflammatory cytokine response when peripheral blood was incubated with lipopolysaccharide alone compared with incubation with clonidine (10-4 M) plus LPS (p > 0.05).
Our results demonstrate that the pre-emptive administration of either clonidine or dexmedetomidine have the ability to successfully improve survival in experimental sepsis. Furthermore, there seems to be a connection between the central muscarinic network and the vagal cholinergic response. By down-regulating pro-inflammatory mediators sympatholytics may be a useful adjunct sedative in patients with a high risk for developing sepsis.
在欧洲和美国的重症监护病房中,死亡的主要原因之一是败血症。它涉及到 TNF-α、IL-1β 和 IL-6 等促炎细胞因子网络。此外,转录因子如核因子(NF)κB 的表达也上调。先前的研究表明,可乐定能够显著降低手术患者的促炎细胞因子。因此,我们假设临床使用的中枢α-2 激动剂可乐定通过抑制交感神经张力并抑制促炎细胞因子释放,从而具有改善实验性败血症患者生存的能力。
为了在一项前瞻性随机实验室研究中研究可乐定的这种治疗潜力,我们使用盲肠结扎和穿刺(CLP)诱导的败血症的小鼠模型。接受预防性注射的动物在手术前 12 小时和 1 小时分别接受可乐定(5μg/kg)或右美托咪定(40μg/kg)治疗,以及术后 1、6 和 12 小时。另一组动物仅在术后 1、6 和 12 小时接受可乐定(5μg/kg)治疗,而预防性注射则为生理盐水。对照组在相应的时间点接受溶剂注射。
中枢交感神经抑制剂的预防性给药显著降低了死亡率(可乐定:p=0.015;右美托咪定:p=0.029),尽管术后给予可乐定未能显著延长生存时间。此外,预防性给予可乐定可显著减轻 CLP 诱导的败血症后的细胞因子反应(mIL-1β:p=0.017;mIL-6:p<0.0001;mTNF-α:p<0.0001),维持血压控制(p=0.024)并下调 NF-κB 的结合活性。与单独用脂多糖孵育相比,当外周血与可乐定(10-4M)加 LPS 孵育时,促炎细胞因子的反应没有变化(p>0.05)。
我们的结果表明,可乐定或右美托咪定的预防性给药均有能力成功改善实验性败血症的生存。此外,中枢毒蕈碱网络和迷走胆碱能反应之间似乎存在联系。通过下调促炎介质,交感神经抑制剂可能是发生败血症风险高的患者有用的辅助镇静剂。