Munier Aline, Diallo Aldiouma, Cot Michel, Ndiaye Ousmane, Arduin Pascal, Chippaux Jean-Philippe
Unité de recherche Santé de la mère et de l'enfant en milieu tropical, IRD UR010, Université Paris Descartes, 4 av de l'Observatoire, 75270 Paris cedex 06, France.
Malar J. 2009 Apr 27;8:83. doi: 10.1186/1475-2875-8-83.
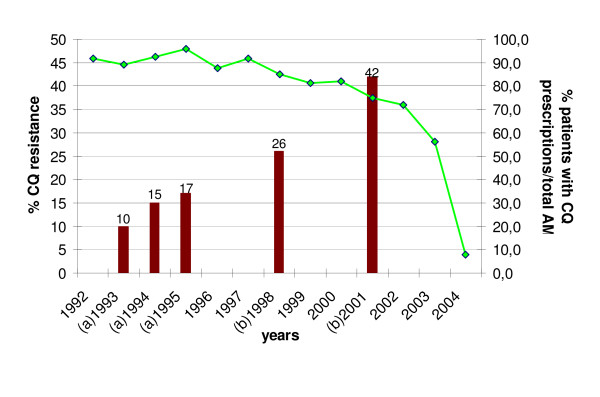
In the rural zone of Niakhar in Senegal, the first therapeutic failures for chloroquine (CQ) were observed in 1992. In 2003, the national policy regarding first-line treatment of uncomplicated malaria was modified, replacing CQ by a transitory bi-therapy amodiaquine/sulphadoxine-pyrimethamine (AQ/SP), before the implementation of artemisinin-based combination therapy (ACT) in 2006. The aims of the study were to assess the evolution of anti-malarial prescriptions in three health care facilities between 1992 and 2004, in parallel with increasing CQ resistance in the region.
The study was conducted in the area of Niakhar, a demographic surveillance site located in a sahelo-sudanese region of Senegal, with mesoendemic and seasonal malaria transmission. Health records of two public health centres and a private catholic dispensary were collected retrospectively to cover the period 1992-2004.
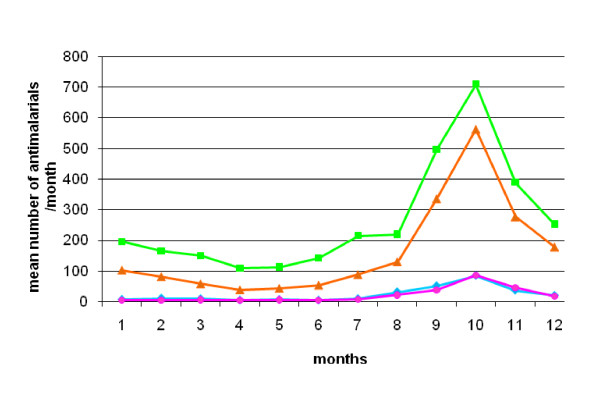
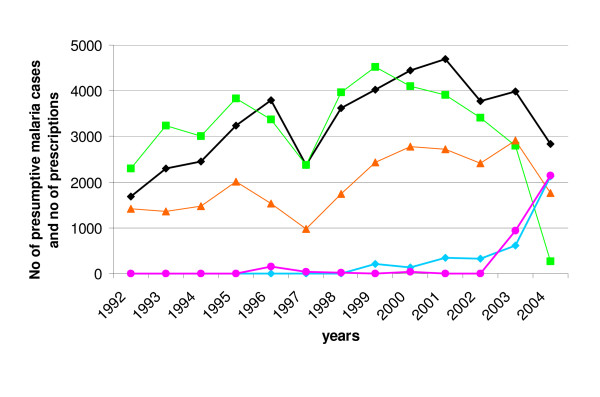
Records included 110,093 consultations and 292,965 prescribed treatments. Twenty-five percent of treatments were anti-malarials, prescribed to 49% of patients. They were delivered all year long, but especially during the rainy season, and 20% of patients with no clinical malaria diagnosis received anti-malarials. Chloroquine and quinine represented respectively 55.7% and 34.6% of prescribed anti-malarials. Overall, chloroquine prescriptions rose from 1992 to 2000, in parallel with clinical malaria; then the CQ prescription rate decreased from 2000 and was concomitant with the rise of SP and the persistence of quinine use. AQ and SP were mainly used as bi-therapy after 2003, at the time of national treatment policy change.
The results show the overall level of anti-malarial prescription in the study area for a considerable number of patients over a large period of time. Even though resistance to CQ rapidly increased from 1992 to 2001, no change in CQ prescription was observed until the early 2000s, possibly due to the absence of an obvious decrease in CQ effectiveness, a lack of therapeutic options or a blind follow-up of national guidelines.
1992年在塞内加尔尼亚喀尔农村地区首次观察到氯喹(CQ)治疗失败的情况。2003年,该国关于单纯性疟疾一线治疗的政策发生了变化,在2006年实施以青蒿素为基础的联合疗法(ACT)之前,采用了临时双药疗法阿莫地喹/磺胺多辛-乙胺嘧啶(AQ/SP)来替代氯喹。本研究的目的是评估1992年至2004年间三个医疗机构抗疟药物处方的演变情况,同时观察该地区氯喹耐药性的增加情况。
本研究在尼亚喀尔地区开展,该地区是位于塞内加尔萨赫勒-苏丹地区的一个人口监测点,疟疾传播呈中度流行且具有季节性。回顾性收集了两个公共卫生中心和一个私立天主教诊所1992 - 2004年期间的健康记录。
记录包括110,093次会诊和292,965次处方治疗。25%的治疗为抗疟药物治疗,49%的患者接受了此类治疗。抗疟药物全年都有开具,但在雨季尤为常见,20%无临床疟疾诊断的患者接受了抗疟药物治疗。氯喹和奎宁分别占所开抗疟药物的55.7%和34.6%。总体而言,氯喹处方量从1992年至2000年随着临床疟疾病例数的增加而上升;然后氯喹处方率从2000年开始下降,同时磺胺多辛-乙胺嘧啶的使用量上升且奎宁的使用持续存在。2003年国家治疗政策改变后,AQ和SP主要作为双药疗法使用。
研究结果显示了在较长一段时间内研究区域内大量患者的抗疟药物处方总体水平。尽管从1992年到2001年对氯喹的耐药性迅速增加,但直到21世纪初氯喹处方量都没有变化,这可能是由于氯喹疗效没有明显下降、缺乏治疗选择或盲目遵循国家指南所致。