Department of Epidemiology and Preventive Medicine, University of Maryland School of Medicine, Baltimore, Maryland, USA.
Malar J. 2009 Jul 15;8:159. doi: 10.1186/1475-2875-8-159.
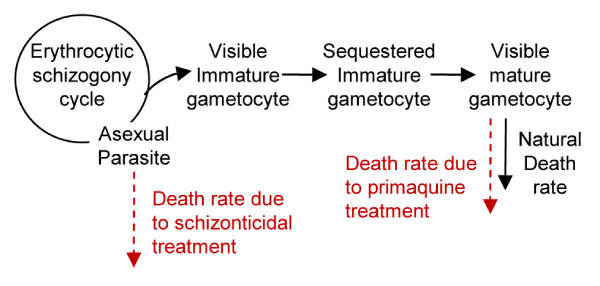
Effective malaria control has successfully reduced the malaria burden in many countries, but to eliminate malaria, these countries will need to further improve their control efforts. Here, a malaria control programme was critically evaluated in a very low-endemicity Thai-Myanmar border population, where early detection and prompt treatment have substantially reduced, though not ended, Plasmodium falciparum transmission, in part due to carriage of late-maturing gametocytes that remain post-treatment. To counter this effect, the WHO recommends the use of a single oral dose of primaquine along with an effective blood schizonticide. However, while the effectiveness of primaquine as a gametocidal agent is widely documented, the mismatch between primaquine's short half-life, the long-delay for gametocyte maturation and the proper timing of primaquine administration have not been studied.
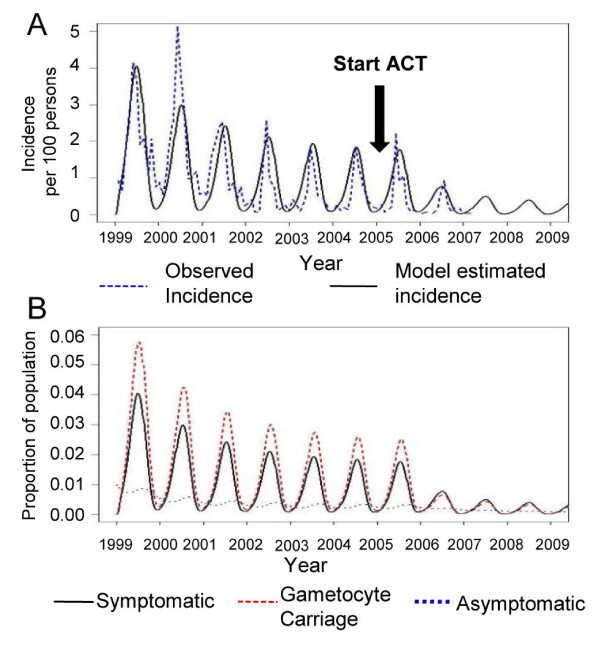
Mathematical models were constructed to simulate 8-year surveillance data, between 1999 and 2006, of seven villages along the Thai-Myanmar border. A simple model was developed to consider primaquine pharmacokinetics and pharmacodynamics, gametocyte carriage, and infectivity.
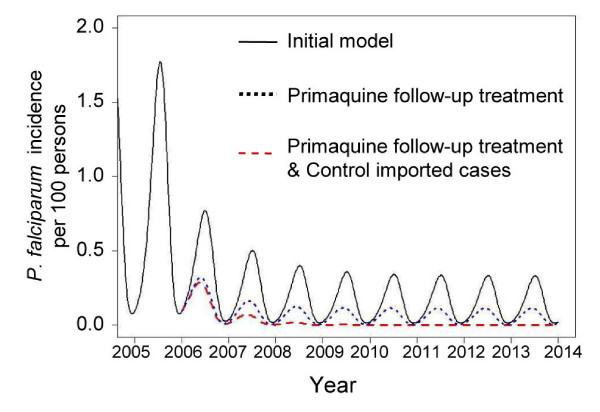
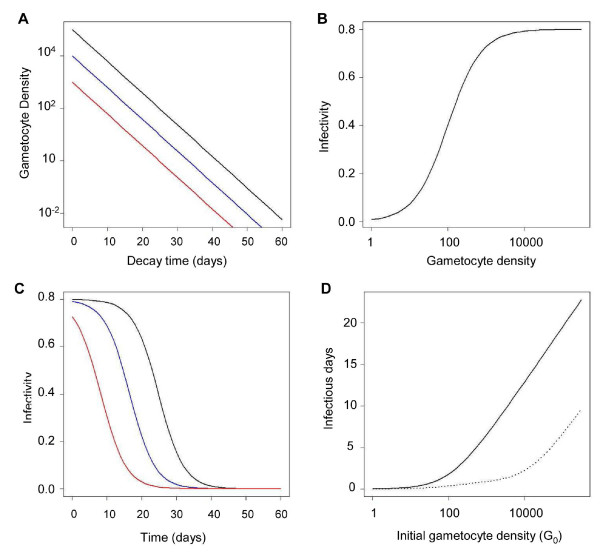
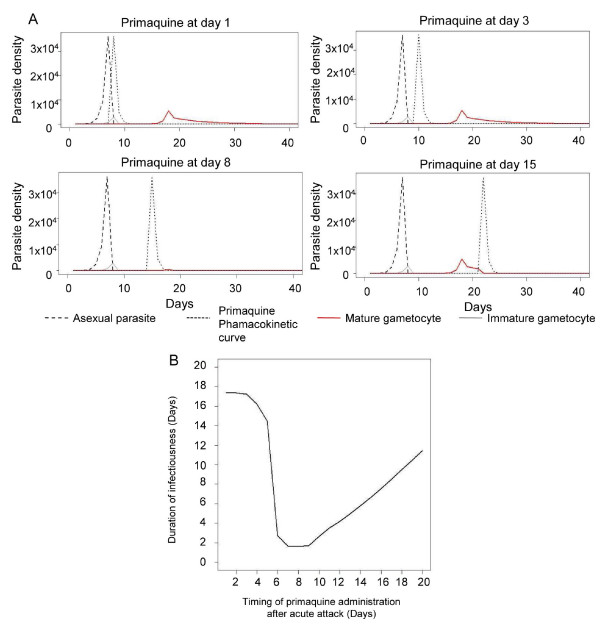
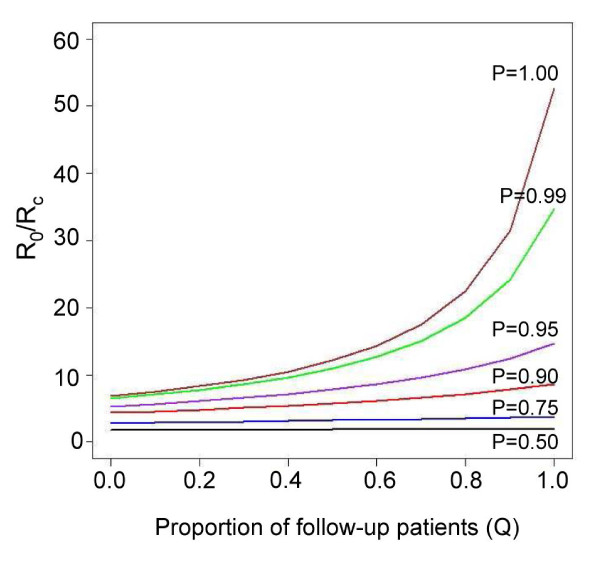
In these populations, transmission intensity is very low, so the P. falciparum parasite rate is strongly linked to imported malaria and to the fraction of cases not treated. Given a 3.6-day half-life of gametocyte, the estimated duration of infectiousness would be reduced by 10 days for every 10-fold reduction in initial gametocyte densities. Infectiousness from mature gametocytes would last two to four weeks and sustain some transmission, depending on the initial parasite densities, but the residual mature gametocytes could be eliminated by primaquine. Because of the short half-life of primaquine (approximately eight hours), it was immediately obvious that with early administration (within three days after an acute attack), primaquine would not be present when mature gametocytes emerged eight days after the appearance of asexual blood-stage parasites. A model of optimal timing suggests that primaquine follow-up approximately eight days after a clinical episode could further reduce the duration of infectiousness from two to four weeks down to a few days. The prospects of malaria elimination would be substantially improved by changing the timing of primaquine administration and combining this with effective detection and management of imported malaria cases. The value of using primaquine to reduce residual gametocyte densities and to reduce malaria transmission was considered in the context of a malaria transmission model; the added benefit of the primaquine follow-up treatment would be relatively large only if a high fraction of patients (>95%) are initially treated with schizonticidal agents.
Mathematical models have previously identified the long duration of P. falciparum asexual blood-stage infections as a critical point in maintaining malaria transmission, but infectiousness can persist for two to four weeks because of residual populations of mature gametocytes. Simulations from new models suggest that, in areas where a large fraction of malaria cases are treated, curing the asexual parasitaemia in a primary infection, and curing mature gametocyte infections with an eight-day follow-up treatment with primaquine have approximately the same proportional effects on reducing the infectious period. Changing the timing of primaquine administration would, in all likelihood, interrupt transmission in this area with very good health systems and with very low endemicity.
有效的疟疾控制已成功降低了许多国家的疟疾负担,但要消除疟疾,这些国家还需要进一步加强控制工作。在这里,在一个疟疾低度流行的泰国-缅甸边境人群中,对疟疾控制项目进行了严格评估,早期发现和及时治疗大大减少了,但并未完全阻断恶性疟原虫的传播,部分原因是携带晚期成熟配子体,治疗后仍存在感染性。为了应对这一影响,世界卫生组织建议使用单一剂量的伯氨喹啉和一种有效的血裂殖体药物。然而,尽管伯氨喹啉作为配子体杀灭剂的有效性已得到广泛证实,但伯氨喹啉半衰期短、配子体成熟延迟以及适当的伯氨喹啉给药时间之间的不匹配尚未得到研究。
构建了数学模型来模拟 1999 年至 2006 年间泰国-缅甸边境七个村庄的八年监测数据。开发了一个简单的模型来考虑伯氨喹啉的药代动力学和药效学、配子体携带和感染力。
在这些人群中,传播强度非常低,因此恶性疟原虫寄生虫率与输入性疟疾和未治疗病例的比例密切相关。如果配子体的半衰期为 3.6 天,那么初始配子体密度每降低 10 倍,估计的传染性就会减少 10 天。成熟配子体的传染性将持续两周至四周,并取决于初始寄生虫密度,但残留的成熟配子体可以通过伯氨喹啉消除。由于伯氨喹啉的半衰期(约 8 小时)很短,因此很明显,如果早期给药(急性发作后三天内),当配子体在出现无性血期寄生虫后八天出现时,伯氨喹啉将不会存在。最佳时间模型表明,在临床发作后大约八天进行伯氨喹啉随访,可以将传染性从两周至四周进一步缩短至几天。改变伯氨喹啉给药时间并结合有效检测和管理输入性疟疾病例,将大大提高消除疟疾的前景。在疟疾传播模型中考虑了使用伯氨喹啉降低残留配子体密度和减少疟疾传播的价值;只有在初始接受裂殖体药物治疗的患者比例较高(>95%)的情况下,伯氨喹啉后续治疗的额外益处才会相对较大。
数学模型以前已经确定了恶性疟原虫无性血期感染的长时间作为维持疟疾传播的关键点,但由于成熟配子体的存在,传染性可持续两周至四周。新模型的模拟结果表明,在疟疾病例的大部分得到治疗的地区,通过对初次感染进行抗疟原虫治疗,以及通过为期八天的伯氨喹啉后续治疗来治愈成熟配子体感染,对减少感染期的影响大致相同。改变伯氨喹啉的给药时间很可能会中断该地区非常好的卫生系统和极低的流行地区的传播。