Ederle Jörg, Bonati Leo H, Dobson Joanna, Featherstone Roland L, Gaines Peter A, Beard Jonathan D, Venables Graham S, Markus Hugh S, Clifton Andrew, Sandercock Peter, Brown Martin M
Stroke Research Group, UCL Institute of Neurology, University College London, Queen Square, London, UK.
Lancet Neurol. 2009 Oct;8(10):898-907. doi: 10.1016/S1474-4422(09)70228-5. Epub 2009 Aug 28.
Endovascular treatment (angioplasty with or without stenting) is an alternative to carotid endarterectomy for carotid artery stenosis but there are scarce long-term efficacy data showing that it prevents stroke. We therefore report the long-term results of the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS).
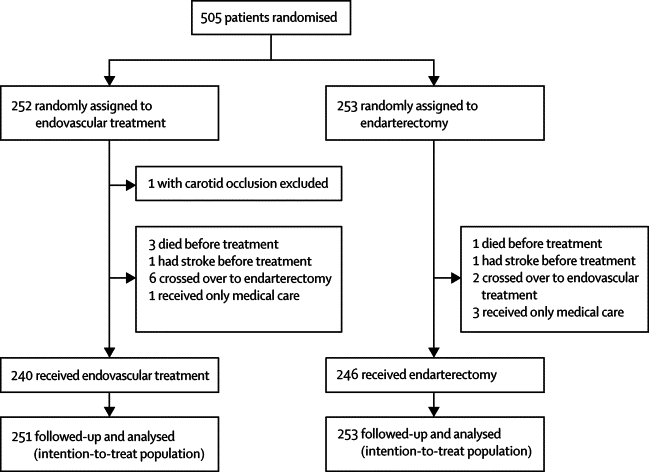
Between March, 1992, and July, 1997, patients who presented at a participating centre with a confirmed stenosis of the internal carotid artery that was deemed equally suitable for either carotid endarterectomy or endovascular treatment were randomly assigned to either treatment in equal proportions by telephone or fax from the randomisation service at the Oxford Clinical Trials Unit, UK. Patients were seen by an independent neurologist at 1 and 6 months after treatment and then every year after randomisation for as long as possible, up to a maximum of 11 years. Major outcome events were transient ischaemic attack, non-disabling, disabling, and fatal stroke, myocardial infarction, and death from any other cause. Outcomes were adjudicated on by investigators who were masked to treatment. Analysis was by intention to treat. This study is registered, number ISRCTN 01425573.
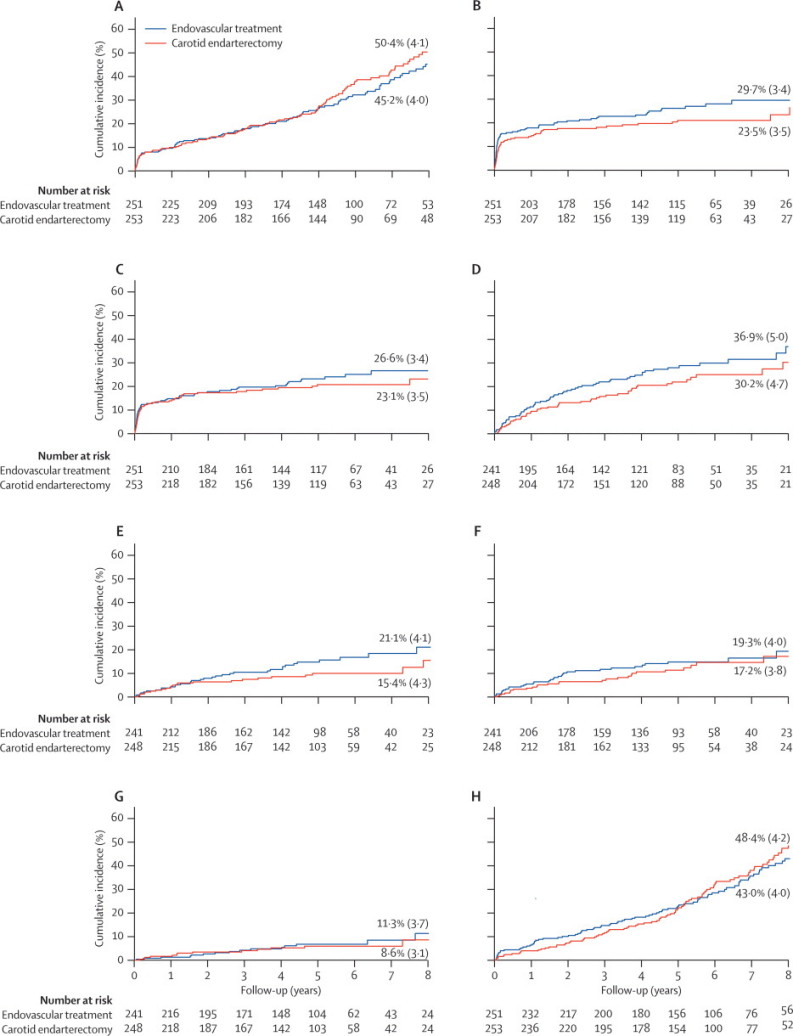
504 patients with stenosis of the carotid artery (90% symptomatic) were randomly assigned to endovascular treatment (n=251) or surgery (n=253). Within 30 days of treatment, there were more minor strokes that lasted less than 7 days in the endovascular group (8 vs 1) but the number of other strokes in any territory or death was the same (25 vs 25). There were more cranial nerve palsies (22 vs 0) in the endarterectomy group than in the endovascular group. Median length of follow up in both groups was 5 years (IQR 2-6). By comparing endovascular treatment with endarterectomy after the 30-day post-treatment period, the 8-year incidence and hazard ratio (HR) at the end of follow-up for ipsilateral non-perioperative stroke was 11.3% versus 8.6% (HR 1.22, 95% CI 0.59-2.54); for ipsilateral non-perioperative stroke or TIA was 19.3% versus 17.2% (1.29, 0.78-2.14); and for any non-perioperative stroke was 21.1% versus 15.4% (1.66, 0.99-2.80).
More patients had stroke during follow-up in the endovascular group than in the surgical group, but the rate of ipsilateral non-perioperative stroke was low in both groups and none of the differences in the stroke outcome measures was significant. However, the study was underpowered and the confidence intervals were wide. More long-term data are needed from the on going stenting versus endarterectomy trials.
British Heart Foundation; UK National Health Service Management Executive; UK Stroke Association.
血管内治疗(血管成形术,可带或不带支架植入)是颈动脉内膜切除术治疗颈动脉狭窄的一种替代方法,但长期疗效数据稀缺,尚无证据表明其可预防中风。因此,我们报告了颈动脉和椎动脉腔内血管成形术研究(CAVATAS)的长期结果。
1992年3月至1997年7月期间,在参与研究的中心就诊且确诊为颈内动脉狭窄、被认为同样适合颈动脉内膜切除术或血管内治疗的患者,通过英国牛津临床试验单位随机服务中心的电话或传真,以相等比例随机分配至两种治疗方法。治疗后1个月和6个月由独立神经科医生进行检查,随机分组后每年尽可能进行检查,最长随访11年。主要结局事件包括短暂性脑缺血发作、非致残性、致残性和致死性中风、心肌梗死以及其他任何原因导致的死亡。结局由对治疗不知情的研究者判定。分析采用意向性分析。本研究的注册号为ISRCTN 01425573。
504例颈动脉狭窄患者(90%有症状)被随机分配至血管内治疗组(n = 251)或手术组(n = 253)。治疗后30天内,血管内治疗组发生持续时间少于7天的轻度中风更多(8例 vs 1例),但其他部位中风或死亡的数量相同(25例 vs 25例)。内膜切除术组的脑神经麻痹更多(22例 vs 0例)。两组的中位随访时间均为5年(四分位间距2 - 6年)。比较治疗后30天的血管内治疗与内膜切除术后,随访结束时同侧非围手术期中风的8年发生率和风险比(HR)分别为11.3%和8.6%(HR 1.22,95%CI 0.59 - 2.54);同侧非围手术期中风或短暂性脑缺血发作的发生率分别为19.3%和17.2%(1.29,0.78 - 2.14);任何非围手术期中风的发生率分别为21.1%和15.4%(1.66,0.99 - 2.80)。
血管内治疗组随访期间发生中风的患者比手术组多,但两组同侧非围手术期中风的发生率均较低,中风结局指标的差异均无统计学意义。然而,该研究效力不足,置信区间较宽。正在进行的支架植入与内膜切除术试验需要更多长期数据。
英国心脏基金会;英国国家卫生服务管理执行委员会;英国中风协会。