Bonati Leo H, Dobson Joanna, Featherstone Roland L, Ederle Jörg, van der Worp H Bart, de Borst Gert J, Mali Willem P Th M, Beard Jonathan D, Cleveland Trevor, Engelter Stefan T, Lyrer Philippe A, Ford Gary A, Dorman Paul J, Brown Martin M
Department of Brain Repair and Rehabilitation, UCL Institute of Neurology, University College London, London, UK; Department of Neurology and Stroke Unit, University Hospital Basel, Basel University, Basel, Switzerland.
Department of Medical Statistics, London School of Hygiene & Tropical Medicine, London, UK.
Lancet. 2015 Feb 7;385(9967):529-38. doi: 10.1016/S0140-6736(14)61184-3. Epub 2014 Oct 14.
Stenting is an alternative to endarterectomy for treatment of carotid artery stenosis, but long-term efficacy is uncertain. We report long-term data from the randomised International Carotid Stenting Study comparison of these treatments.
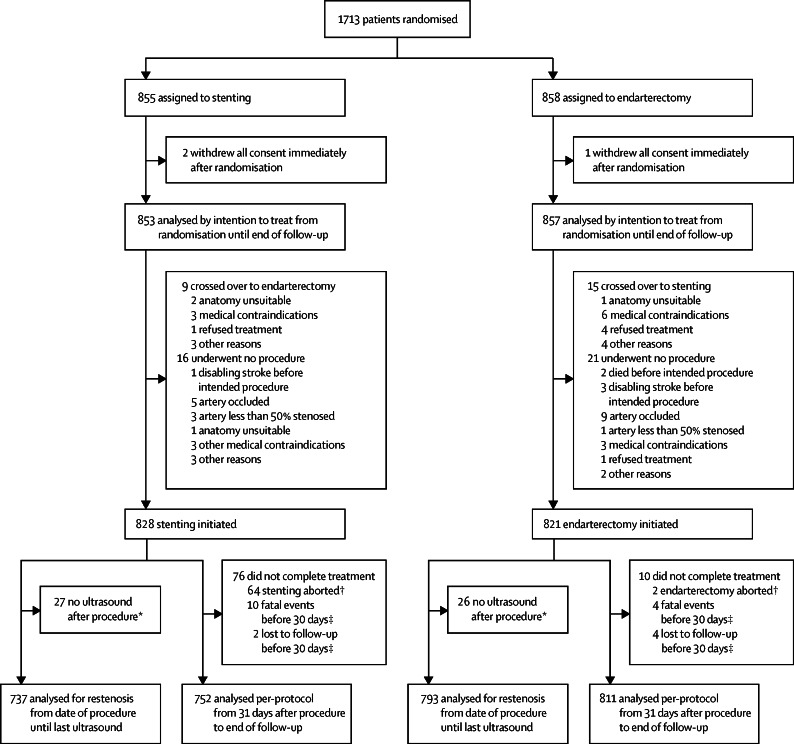
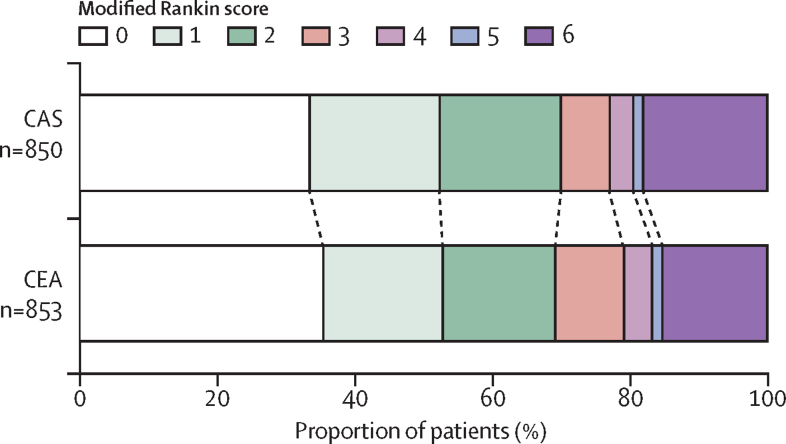
Patients with symptomatic carotid stenosis were randomly assigned 1:1 to open treatment with stenting or endarterectomy at 50 centres worldwide. Randomisation was computer generated centrally and allocated by telephone call or fax. Major outcomes were assessed by an independent endpoint committee unaware of treatment assignment. The primary endpoint was fatal or disabling stroke in any territory after randomisation to the end of follow-up. Analysis was by intention to treat ([ITT] all patients) and per protocol from 31 days after treatment (all patients in whom assigned treatment was completed). Functional ability was rated with the modified Rankin scale. This study is registered, number ISRCTN25337470.
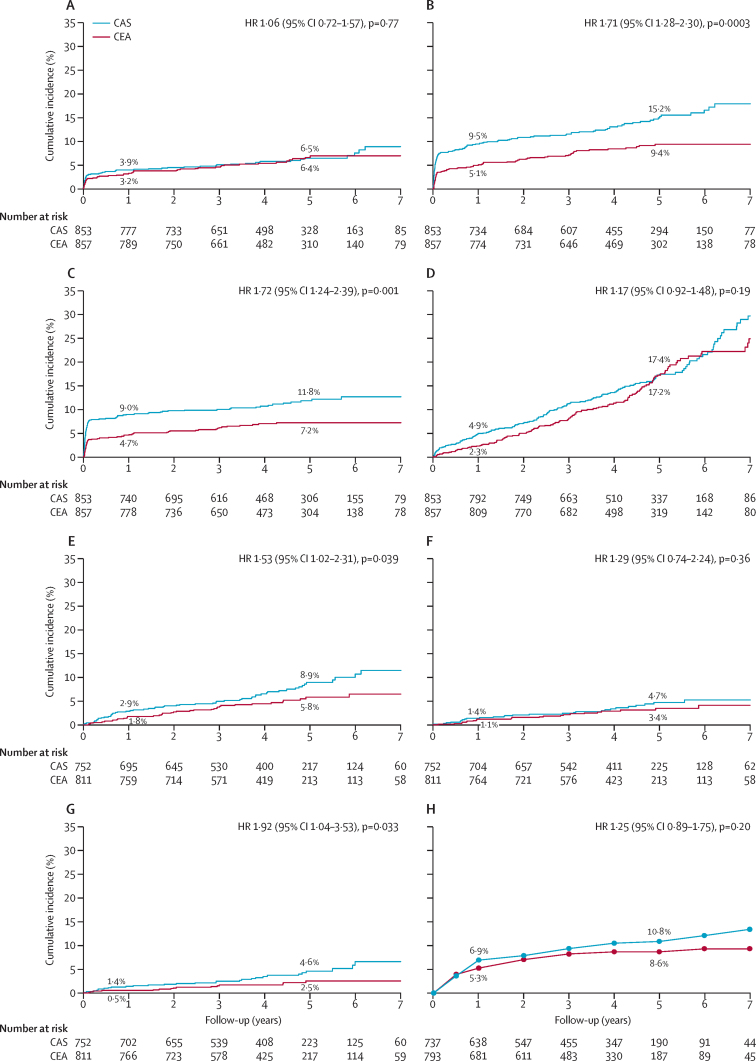
1713 patients were assigned to stenting (n=855) or endarterectomy (n=858) and followed up for a median of 4·2 years (IQR 3·0-5·2, maximum 10·0). Three patients withdrew immediately and, therefore, the ITT population comprised 1710 patients. The number of fatal or disabling strokes (52 vs 49) and cumulative 5-year risk did not differ significantly between the stenting and endarterectomy groups (6·4% vs 6·5%; hazard ratio [HR] 1·06, 95% CI 0·72-1·57, p=0·77). Any stroke was more frequent in the stenting group than in the endarterectomy group (119 vs 72 events; ITT population, 5-year cumulative risk 15·2% vs 9·4%, HR 1·71, 95% CI 1·28-2·30, p<0·001; per-protocol population, 5-year cumulative risk 8·9% vs 5·8%, 1·53, 1·02-2·31, p=0·04), but were mainly non-disabling strokes. The distribution of modified Rankin scale scores at 1 year, 5 years, or final follow-up did not differ significantly between treatment groups.
Long-term functional outcome and risk of fatal or disabling stroke are similar for stenting and endarterectomy for symptomatic carotid stenosis.
Medical Research Council, Stroke Association, Sanofi-Synthélabo, European Union.
支架置入术是治疗颈动脉狭窄的一种替代动脉内膜切除术的方法,但长期疗效尚不确定。我们报告了这些治疗方法随机对照的国际颈动脉支架置入研究的长期数据。
有症状的颈动脉狭窄患者在全球50个中心按1:1随机分配接受支架置入术或动脉内膜切除术的开放治疗。随机分组由中央计算机生成,并通过电话或传真进行分配。主要结局由一个不知道治疗分配情况的独立终点委员会评估。主要终点是随机分组后至随访结束在任何区域发生的致死性或致残性卒中。分析采用意向性分析([ITT]所有患者)和治疗后31天起的符合方案分析(所有完成指定治疗的患者)。功能能力用改良Rankin量表评定。本研究已注册,注册号为ISRCTN25337470。
1713例患者被分配接受支架置入术(n = 855)或动脉内膜切除术(n = 858),中位随访时间为4.2年(IQR 3.0 - 5.2,最长10.0年)。3例患者立即退出,因此ITT人群包括1710例患者。支架置入术组和动脉内膜切除术组的致死性或致残性卒中数量(分别为52例和49例)及5年累积风险无显著差异(6.4%对6.5%;风险比[HR]1.06,95%CI 0.72 - 1.57,p = 0.77)。支架置入术组的任何卒中发生率高于动脉内膜切除术组(分别为119例和72例事件;ITT人群,5年累积风险15.2%对9.4%,HR 1.71,95%CI 1.28 - 2.30,p<0.001;符合方案人群,5年累积风险8.9%对5.8%,1.53,1.02 - 2.31,p = 0.04),但主要是非致残性卒中。治疗组在1年、5年或最终随访时改良Rankin量表评分分布无显著差异。
对于有症状的颈动脉狭窄,支架置入术和动脉内膜切除术的长期功能结局以及致死性或致残性卒中风险相似。
医学研究理事会、卒中协会、赛诺菲 - 圣德拉堡公司、欧盟。