Department of Neuroscience, Intensive Care Unit, Marche Polytechnical University, Via Tronto 10/A, 60020 Torrette di Ancona, Italy.
Crit Care. 2009;13 Suppl 5(Suppl 5):S12. doi: 10.1186/cc8010. Epub 2009 Nov 30.
The purpose was to test the hypothesis that muscle perfusion, oxygenation, and microvascular reactivity would improve in patients with severe sepsis or septic shock during treatment with recombinant activated protein C (rh-aPC) (n = 11) and to explore whether these parameters are related to macrohemodynamic indices, metabolic status or Sequential Organ Failure Assessment (SOFA) score. Patients with contraindications to rh-aPC were used as a control group (n = 5).
Patients were sedated, intubated, mechanically ventilated, and hemodynamically monitored with the PiCCO system. Tissue oxygen saturation (StO2) was measured using near-infrared spectroscopy (NIRS) during the vascular occlusion test (VOT). Baseline StO2 (StO2 baseline), rate of decrease in StO2 during VOT (StO2 downslope), and rate of increase in StO2 during the reperfusion phase were (StO2 upslope) determined. Data were collected before (T0), during (24 hours (T1a), 48 hours (T1b), 72 hours (T1c) and 96 hours (T1d)) and 6 hours after stopping rh-aPC treatment (T2) and at the same times in the controls. At every assessment, hemodynamic and metabolic parameters were registered and the SOFA score calculated.
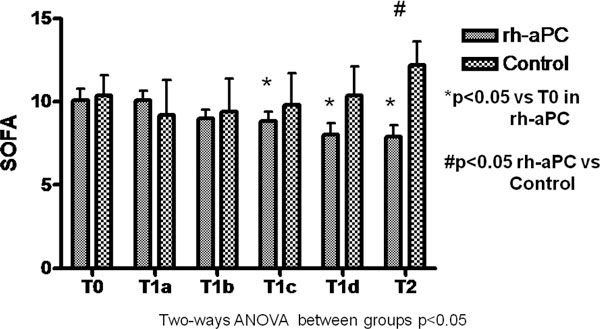
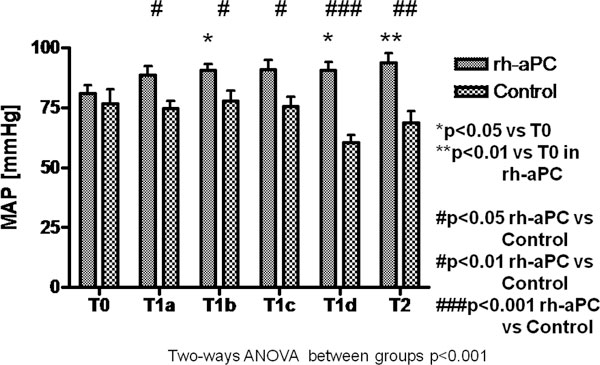
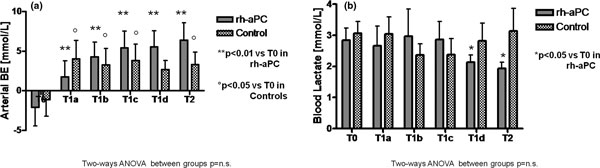
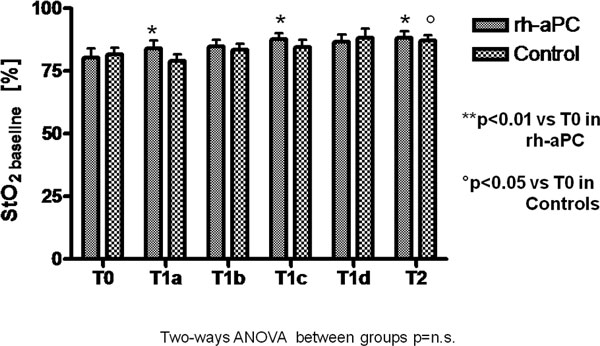
The mean +/- standard deviation Acute Physiology and Chronic Health Evaluation II score was 26.3 +/- 6.6 and 28.6 +/- 5.3 in rh-aPC and control groups, respectively. There were no significant differences in macrohemodynamic parameters between the groups at all the time points. In the rh-aPC group, base excess was corrected (P < 0.01) from T1a until T2, and blood lactate was significantly decreased at T1d and T2 (2.8 +/- 1.3 vs. 1.9 +/- 0.7 mmol/l; P < 0.05). In the control group, base excess was significantly corrected at T1a, T1b, T1c, and T2 (P < 0.05). The SOFA score was significantly lower in the rh-aPC group compared with the controls at T2 (7.9 +/- 2.2 vs. 12.2 +/- 3.2; P < 0.05). There were no differences between groups in StO2 baseline. StO2 downslope in the rh-aPC group decreased significantly at all the time points, and at T1b and T2 (-16.5 +/- 11.8 vs. -8.1 +/- 2.4%/minute) was significantly steeper than in the control group. StO2 upslope increased and was higher than in the control group at T1c, T1d and T2 (101.1 +/- 62.1 vs. 54.5 +/- 23.8%/minute) (P < 0.05).
Treatment with rh-aPC may improve muscle oxygenation (StO2 baseline) and reperfusion (StO2 upslope) and, furthermore, rh-aPC treatment may increase tissue metabolism (StO2 downslope). NIRS is a simple, real-time, non-invasive technique that could be used to monitor the effects of rh-aPC therapy at microcirculatory level in septic patients.
目的是检验以下假设,即在严重脓毒症或感染性休克患者中使用重组活化蛋白 C(rh-aPC)治疗时,肌肉灌注、氧合和微血管反应性会得到改善,并探讨这些参数是否与宏观血流动力学指标、代谢状态或序贯器官衰竭评估(SOFA)评分有关。使用 rh-aPC 禁忌的患者作为对照组(n=5)。
患者接受镇静、插管、机械通气,并使用脉搏指示剂连续心排血量(PiCCO)系统进行血流动力学监测。在血管闭塞试验(VOT)期间使用近红外光谱(NIRS)测量组织氧饱和度(StO2)。在基线(StO2 baseline)时、VOT 期间 StO2 下降速度(StO2 downslope)和再灌注期 StO2 上升速度(StO2 upslope)确定。在 rh-aPC 治疗前(T0)、治疗期间(24 小时(T1a)、48 小时(T1b)、72 小时(T1c)和 96 小时(T1d))和治疗停止后 6 小时(T2)以及对照组的相同时间收集数据。在每次评估时,记录血流动力学和代谢参数,并计算 SOFA 评分。
rh-aPC 和对照组的急性生理学和慢性健康评估 II 评分平均值±标准差分别为 26.3±6.6 和 28.6±5.3。两组在所有时间点的宏观血流动力学参数均无显著差异。在 rh-aPC 组中,从 T1a 到 T2 时碱剩余得到纠正(P<0.01),并且在 T1d 和 T2 时血乳酸明显降低(2.8±1.3 vs. 1.9±0.7 mmol/l;P<0.05)。在对照组中,碱剩余在 T1a、T1b、T1c 和 T2 时均得到显著纠正(P<0.05)。与对照组相比,rh-aPC 组在 T2 时 SOFA 评分显著降低(7.9±2.2 vs. 12.2±3.2;P<0.05)。两组间 StO2 baseline 无差异。rh-aPC 组在所有时间点的 StO2 downslope 均显著下降,并且在 T1b 和 T2 时(-16.5±11.8 vs. -8.1±2.4%/分钟)斜率明显比对照组陡峭。在 T1c、T1d 和 T2 时,StO2 upslope 增加且高于对照组(101.1±62.1 vs. 54.5±23.8%/分钟)(P<0.05)。
rh-aPC 治疗可能改善肌肉氧合(StO2 baseline)和再灌注(StO2 upslope),并且 rh-aPC 治疗可能增加组织代谢(StO2 downslope)。NIRS 是一种简单、实时、非侵入性的技术,可用于监测感染性休克患者 rh-aPC 治疗的微循环效果。