Department of Critical Care Medicine, University of Pittsburgh, 606 Scaife Hall, 3550 Terrace Street, Pittsburgh, PA 15261, USA.
Crit Care. 2009;13 Suppl 5(Suppl 5):S3. doi: 10.1186/cc8001. Epub 2009 Nov 30.
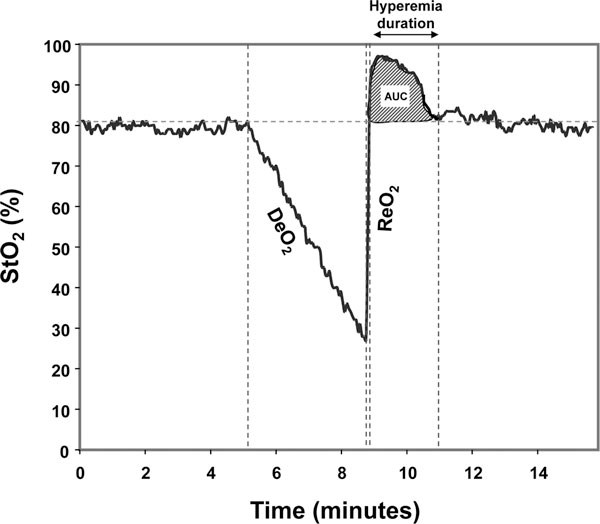
Tissue oxygen saturation (StO2) and the vascular occlusion test (VOT) can identify tissue hypoperfusion in trauma and sepsis. However, the technique is neither standardized nor uses the same monitoring site. We hypothesized that baseline and VOT StO2 would be different in the forearm (F) and thenar eminence (TH) and that different minimal StO2 values during the VOT would result in different reoxygenation rates (ReO2).
StO2 and its change during the VOT were simultaneously measured in the F and TH, with 15 mm and 25 mm probes, using the 325 InSpectra monitor in 18 healthy, adult volunteers. Two VOTs were done to a threshold thenar StO2 of 40% interchanging the 15 mm and 25 mm probes between sites. Two additional VOTs were done to thresholds of 50% and 30%. Baseline StO2 (BaseO2), the deoxygenation rate (DeO2) and ReO2 were compared between sites, probes and (%O2/minute) thresholds. Results are presented as the median (interquartile range), P-value.
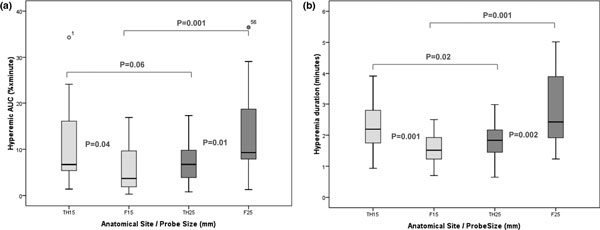
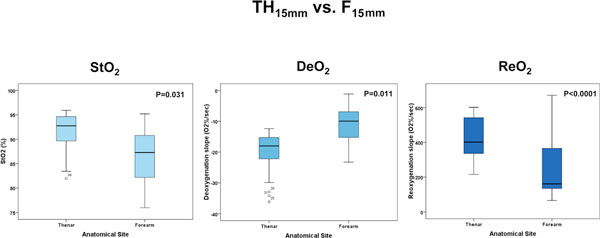
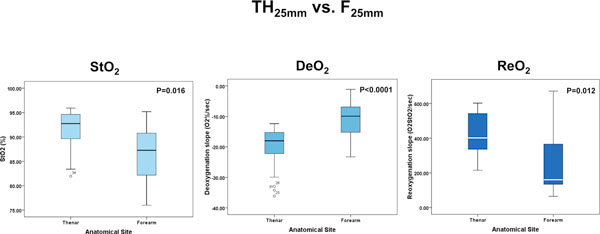
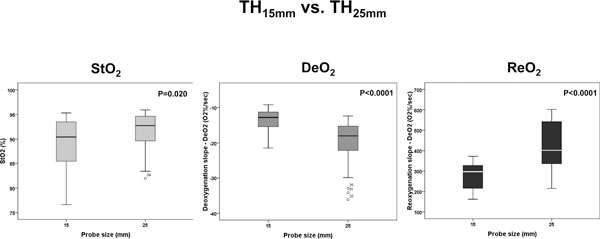
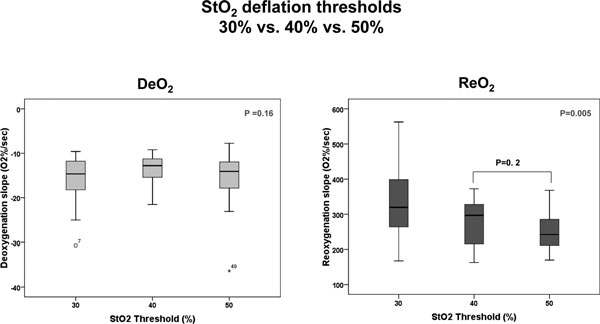
BaseO2, DeO2, ReO2, area under the curve and hyperemia duration values were different when comparing TH vs. F and 15 mm vs. 25 mm probes. ReO2 was different between different thresholds for the TH and 15 mm probes. TH15 mm vs. F15 mm: BaseO2, 90.4 (85.2, 93.5) vs. 85.2 (80.7, 90.2), P = 0.031; DO2, -12.1 (-16.2, -11.3) vs. -8.5 (-10.3, -7.8), P = 0.011; ReO2, 297.2 (213.7, 328.6), P < 0.0001; 15 mm vs. 25 mm probe: BaseO2, 97.2 (89.4, 94.7) vs. 87.3 (81.7, 90.9), P = 0.016; DeO2, -18.0 (-24.1, -14.8) vs. -9.9 (-15.3, -6.5), P < 0.0001; and ReO2, 401.6 (331.7, 543.2) vs. 160.5 (132.3, 366.9), P = 0.012, respectively. TH15 mm vs. TH25 mm: BaseO2, P = 0.020; DeO2, P < 0.0001; and ReO2, P < 0.0001. Threshold StO2 values (15 mm probe only): ReO2, P = 0.003; DeO2, P = 0.60. ReO2 at 40% and 50% StO2 thresholds, P = 0.01.
BaseO2, DeO2 and ReO2 were different when measured in different anatomical sites (F and TH) and with different probe sizes, and ReO2 was different with differing VOT release StO2 threshold values. Thus, standardization of the site, probe and VOT challenge need to be stipulated when reporting data.
组织氧饱和度(StO2)和血管闭塞试验(VOT)可识别创伤和脓毒症中的组织灌注不足。然而,该技术既没有标准化,也没有使用相同的监测部位。我们假设在创伤和脓毒症中,前臂(F)和鱼际(TH)的基线和 VOT StO2 不同,并且 VOT 期间不同的最小 StO2 值会导致不同的再氧合率(ReO2)。
使用 325 InSpectra 监测仪,在 18 名健康成年志愿者中,使用 15 毫米和 25 毫米探头,同时测量 F 和 TH 中的 StO2 及其在 VOT 期间的变化。进行了两次 VOT,阈值为 THENAR StO2 为 40%,在两个部位之间交换 15 毫米和 25 毫米探头。另外进行了两次 VOT,阈值为 50%和 30%。比较了部位、探头和(%O2/minute)阈值之间的基线 StO2(BaseO2)、脱氧率(DeO2)和再氧合率(ReO2)。结果以中位数(四分位距)表示,P 值。
TH 与 F 和 15 毫米与 25 毫米探头比较时,BaseO2、DeO2、ReO2、曲线下面积和充血持续时间值不同。TH 和 15 毫米探头的不同阈值之间的 ReO2 不同。TH15 毫米与 F15 毫米:BaseO2,90.4(85.2,93.5)与 85.2(80.7,90.2),P=0.031;DO2,-12.1(-16.2,-11.3)与-8.5(-10.3,-7.8),P=0.011;ReO2,297.2(213.7,328.6),P <0.0001;15 毫米与 25 毫米探头:BaseO2,97.2(89.4,94.7)与 87.3(81.7,90.9),P=0.016;DeO2,-18.0(-24.1,-14.8)与-9.9(-15.3,-6.5),P <0.0001;ReO2,401.6(331.7,543.2)与 160.5(132.3,366.9),P=0.012,分别。TH15 毫米与 TH25 毫米:BaseO2,P=0.020;DeO2,P <0.0001;ReO2,P <0.0001。阈值 StO2 值(仅 15 毫米探头):ReO2,P=0.003;DeO2,P=0.60。40%和 50% StO2 阈值的 ReO2,P=0.01。
当在不同的解剖部位(F 和 TH)和不同的探头尺寸进行测量时,BaseO2、DeO2 和 ReO2 不同,并且随着 VOT 释放 StO2 阈值的不同,ReO2 也不同。因此,在报告数据时需要规定部位、探头和 VOT 挑战的标准化。