Hypertension and Vascular Research Center, Wake Forest University School of Medicine, Medical Center Boulevard, Winston-Salem, NC 27157-1032, United States.
Life Sci. 2010 Feb 27;86(9-10):289-99. doi: 10.1016/j.lfs.2009.11.020. Epub 2009 Dec 1.
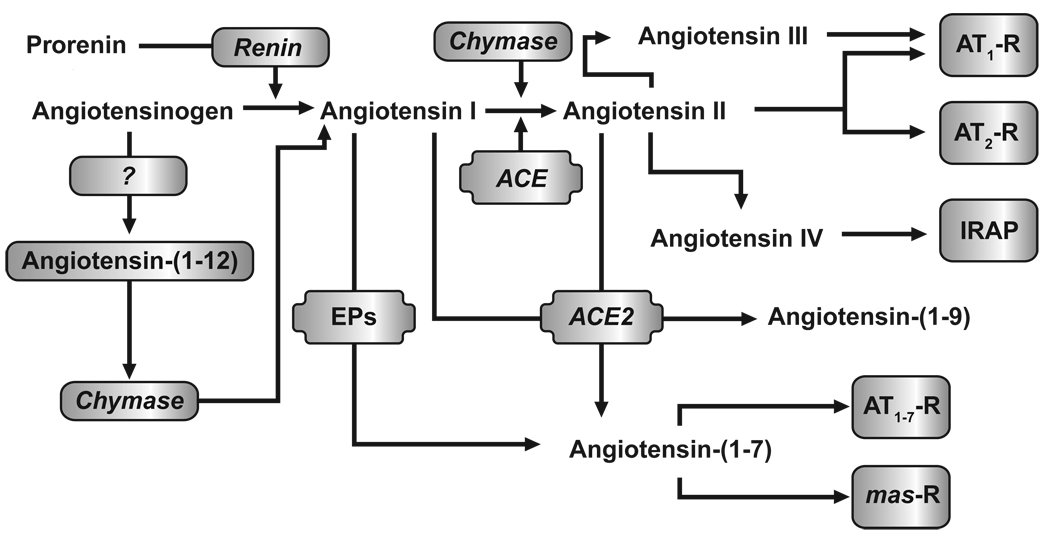
This article reviews the importance of the renin-angiotensin-aldosterone system (RAAS) in the cardiometabolic continuum; presents the pros and cons of dual RAAS blockade with angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs); and examines the theoretical and practical benefits supporting the use of direct renin inhibitors (DRIs) in combination with ACEIs or ARBs.
The author reviewed the literature for key publications related to the biochemical physiology of the RAAS and the pharmacodynamic effects of ACEIs, ARBs, and DRIs, with a particular focus on dual RAAS blockade with these drug classes.
Although ACEI/ARB combination therapy produces modest improvement in BP, it has not resulted in the major improvements predicted given the importance of the RAAS across the cardiorenal disease continuum. This may reflect the fact that RAAS blockade with ACEIs and/or ARBs leads to exacerbated renin release through loss of negative-feedback inhibition, as well as ACE/aldosterone escape through RAAS and non-RAAS-mediated mechanisms. Plasma renin activity (PRA) is an independent predictor of morbidity and mortality, even for patients receiving ACEIs and ARBs. When used alone or in combination with ACEIs and ARBs, the DRI aliskiren effectively reduces PRA. Reductions in BP are greater with these combinations, relative to the individual components alone.
It is possible that aliskiren plus either an ACEI or ARB may provide greater RAAS blockade than monotherapy with ACEIs or ARBs, and lead to additive improvement in BP and clinically important outcomes.
本文回顾了肾素-血管紧张素-醛固酮系统(RAAS)在心脏代谢连续统中的重要性;介绍了血管紧张素转换酶抑制剂(ACEI)和血管紧张素受体阻滞剂(ARB)联合双重 RAAS 阻断的优缺点;并探讨了支持直接肾素抑制剂(DRI)与 ACEI 或 ARB 联合使用的理论和实际益处。
作者回顾了与 RAAS 的生化生理学和 ACEI、ARB 和 DRI 的药效学相关的关键文献,特别关注这些药物类别联合进行双重 RAAS 阻断。
尽管 ACEI/ARB 联合治疗可使血压适度改善,但并未如 RAAS 在心脏肾脏疾病连续统中的重要性所预测的那样取得重大改善。这可能反映了 ACEI 和/或 ARB 阻断 RAAS 会导致肾素释放加剧,这是由于负反馈抑制丧失,以及通过 RAAS 和非 RAAS 介导的机制导致 ACE/醛固酮逃逸。血浆肾素活性(PRA)是发病率和死亡率的独立预测因素,即使患者正在接受 ACEI 和 ARB 治疗也是如此。当单独使用或与 ACEI 和 ARB 联合使用时,DRI 阿利吉仑可有效降低 PRA。与单独使用这些药物相比,这些组合可使血压降低更明显。
阿利吉仑加用 ACEI 或 ARB 可能比单独使用 ACEI 或 ARB 进行单一疗法提供更大的 RAAS 阻断,并导致血压和临床重要结局的附加改善。