Service de Réanimation Médicale, Groupe Hospitalier Pitié-Salpêtrière, Assistance Publique-Hôpitaux de Paris, Université Paris-Pierre-et-Marie-Curie, 75651 Paris Cedex 13, France.
Crit Care. 2009;13(6):R200. doi: 10.1186/cc8206. Epub 2009 Dec 10.
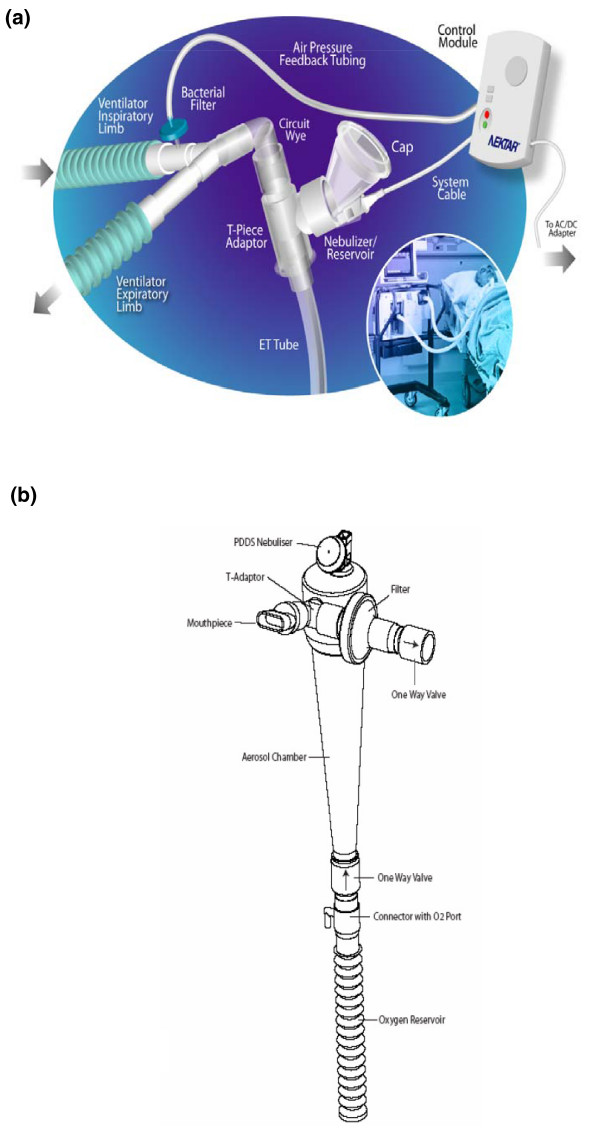
Aminoglycosides aerosolization might achieve better diffusion into the alveolar compartment than intravenous use. The objective of this multicenter study was to evaluate aerosol-delivered amikacin penetration into the alveolar epithelial lining fluid (ELF) using a new vibrating mesh nebulizer (Pulmonary Drug Delivery System (PDDS), Nektar Therapeutics), which delivers high doses to the lungs.
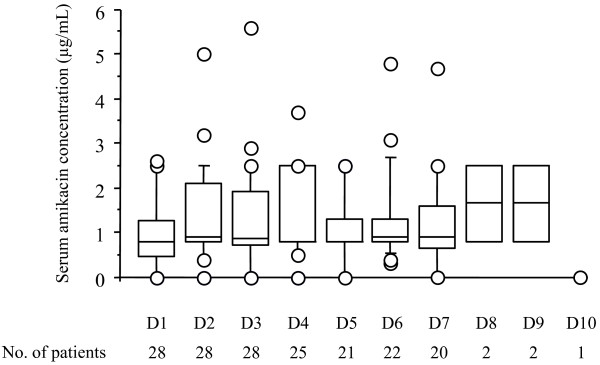
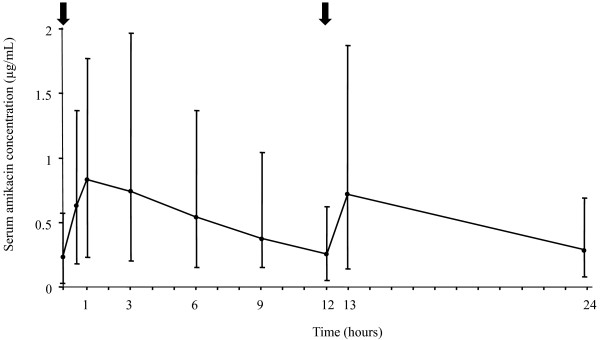
Nebulized amikacin (400 mg bid) was delivered to the lungs of 28 mechanically ventilated patients with Gram-negative VAP for 7-14 days, adjunctive to intravenous therapy. On treatment day 3, 30 minutes after completing aerosol delivery, all the patients underwent bronchoalveolar lavage in the infection-involved area and the ELF amikacin concentration was determined. The same day, urine and serum amikacin concentrations were determined at different time points.
Median (range) ELF amikacin and maximum serum amikacin concentrations were 976.1 (135.7-16127.6) and 0.9 (0.62-1.73) microg/mL, respectively. The median total amount of amikacin excreted in urine during the first and second 12-hour collection on day 3 were 19 (12.21-28) and 21.2 (14.1-29.98) microg, respectively. During the study period, daily through amikacin measurements were below the level of nephrotoxicity. Sixty-four unexpected adverse events were reported, among which 2 were deemed possibly due to nebulized amikacin: one episode of worsening renal failure, and one episode of bronchospasm.
PDDS delivery of aerosolized amikacin achieved very high aminoglycoside concentrations in ELF from radiography-controlled infection-involved zones, while maintaining safe serum amikacin concentrations. The ELF concentrations always exceeded the amikacin minimum inhibitory concentrations for Gram-negative microorganisms usually responsible for these pneumonias. The clinical impact of amikacin delivery with this system remains to be determined.
ClinicalTrials.gov Identifier: NCT01021436.
氨基糖苷类药物雾化吸入比静脉使用可能具有更好的肺泡扩散作用。本多中心研究的目的是使用新型振动网孔雾化器(Pulmonary Drug Delivery System (PDDS),Nektar Therapeutics)评估雾化吸入阿米卡星穿透肺泡上皮衬液(ELF)的情况,该装置可向肺部输送高剂量药物。
28 例革兰氏阴性菌 VAP 机械通气患者接受雾化阿米卡星(400mg,bid)治疗 7-14 天,辅助静脉治疗。在治疗第 3 天,气溶胶输送完成后 30 分钟,所有患者在感染受累区域进行支气管肺泡灌洗,并测定 ELF 阿米卡星浓度。同日,在不同时间点测定尿液和血清阿米卡星浓度。
中位(范围)ELF 阿米卡星和最大血清阿米卡星浓度分别为 976.1(135.7-16127.6)和 0.9(0.62-1.73)μg/mL。第 3 天第 1 和第 2 个 12 小时收集尿液中阿米卡星的中位排泄总量分别为 19(12.21-28)和 21.2(14.1-29.98)μg。在研究期间,每日通过阿米卡星测量值均低于肾毒性水平。报告了 64 例意外不良事件,其中 2 例被认为可能与雾化阿米卡星有关:1 例肾功能衰竭恶化,1 例支气管痉挛。
PDDS 输送雾化阿米卡星可在影像学控制的感染受累区域的 ELF 中实现非常高的氨基糖苷类浓度,同时保持安全的血清阿米卡星浓度。ELF 浓度始终超过通常导致这些肺炎的革兰氏阴性微生物的阿米卡星最小抑菌浓度。该系统输送阿米卡星的临床影响仍有待确定。
ClinicalTrials.gov 标识符:NCT01021436。