Presanis Anne M, Lipsitch Marc, Hagy Angie, Reed Carrie, Riley Steven, Cooper Ben, Biedrzycki Paul, Finelli Lyn, B Jade
MRC Biostatistics Unit, Cambridge; Dept of Epidemiology and Center for Communicable Disease Dynamics, Harvard School of Public Health; Health Protection Agency, London and MRC Biostatistics Unit, Cambridge; City of Milwaukee Health Department; Epidemiologist, Centers for Disease Control and Prevention; The University of Hong Kong; Health Protection Agency and CDC.
PLoS Curr. 2009 Sep 25;1:RRN1042. doi: 10.1371/currents.RRN1042.
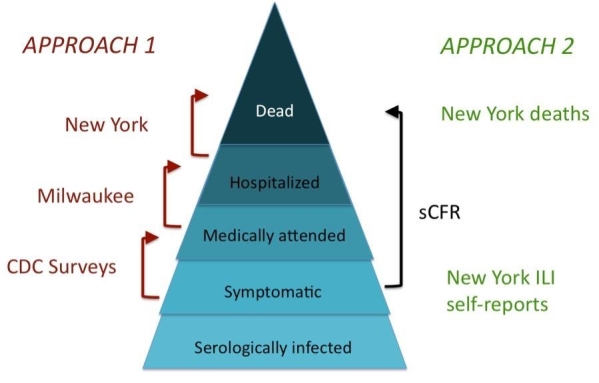
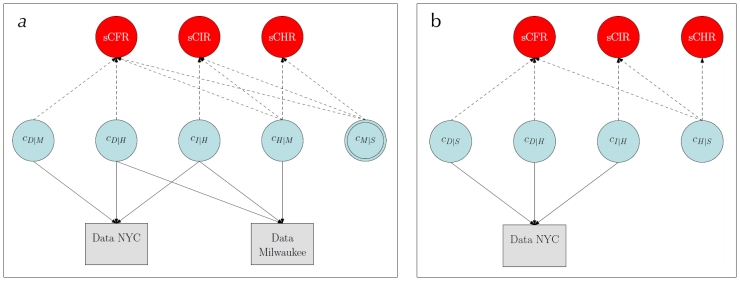
BackgroundAccurate measures of the severity of pandemic influenza A/H1N1 (pH1N1) are needed to assess the likely impact of an anticipated resurgence in the autumn in the Northern Hemisphere. Severity has been difficult to measure because jurisdictions with large numbers of deaths and other severe outcomes have had too many cases to assess the total number with confidence. Also, detection of severe cases may be more likely. Methods and FindingsWe used complementary data from two US cities: Milwaukee attempted to identify cases of medically attended infection whether or not they required hospitalization, while New York City focused on the identification of hospitalizations, intensive care admission or mechanical ventilation (hereafter, ICU), and deaths. New York data were used to estimate numerators for ICU and death, and two sources of data: medically attended cases in Milwaukee or self-reported influenza-like illness in New York, were used to estimate ratios of symptomatic cases:hospitalizations. Combining these data with estimates of the fraction detected for each level of severity, we estimated the proportion of symptomatic cases that died (symptomatic case-fatality ratio, sCFR), required ICU (sCIR), and required hospitalization (sCHR), overall and by age category. Evidence, prior information and associated uncertainty were analyzed in a Bayesian evidence synthesis framework. Using medically attended cases and estimates of the proportion of symptomatic cases medically attended, we estimated sCFR of 0.048% (95% credible interval, CI 0.026%-0.096%), sCIR of 0.239% (0.134%-0.458%), and sCHR of 1.44% (0.83%-2.64%). Using self-reported ILI, we obtained estimates approximately 7-9x lower. sCFR and sCIR appear to be highest in persons 18 and older, and lowest in children 5-17. sCHR appears to be lowest in persons 5-17; our data were too sparse to allow us to determine the group in which it was the highest. ConclusionsThese estimates suggest that an autumn-winter pandemic wave of pH1N1 with comparable severity per case could lead to a number of deaths in the range from considerably below that associated with seasonal influenza to slightly higher, but with greatest impact in young children and non-elderly adults. These estimates of impact depend on assumptions about total incidence of infection and would be larger if incidence of symptomatic infection were higher or shifted toward adults, if viral virulence increased, or if suboptimal treatment resulted from stress on the health care system; numbers would decrease if the proportion infected or symptomatic were lower.
背景
为评估北半球秋季甲型H1N1流感大流行(pH1N1)预计卷土重来可能产生的影响,需要准确衡量其严重程度。由于死亡人数众多及出现其他严重后果的辖区病例过多,难以确切评估总数,因此严重程度一直难以衡量。此外,严重病例可能更易被发现。
方法与发现
密尔沃基试图识别接受医疗护理的感染病例,无论是否需要住院治疗;而纽约市则专注于识别住院、重症监护病房收治或机械通气(以下简称ICU)以及死亡病例。纽约的数据用于估计ICU和死亡病例的分子,密尔沃基接受医疗护理的病例或纽约自我报告的流感样疾病这两个数据源用于估计有症状病例与住院病例的比率。将这些数据与每个严重程度水平的检测比例估计值相结合,我们估计了有症状病例死亡(有症状病例病死率,sCFR)、需要ICU(有症状病例重症监护率,sCIR)和需要住院(有症状病例住院率,sCHR)的比例,整体及按年龄类别分别进行了估计。在贝叶斯证据综合框架下分析了证据、先验信息及相关不确定性。利用接受医疗护理的病例及接受医疗护理的有症状病例比例估计值,我们估计sCFR为0.048%(95%可信区间,CI 0.026% - 0.096%),sCIR为0.239%(0.134% - 0.458%),sCHR为1.44%(0.83% - 2.64%)。利用自我报告的流感样疾病数据,我们得到的估计值约低7 - 9倍。sCFR和sCIR似乎在18岁及以上人群中最高,在5 - <17岁儿童中最低。sCHR似乎在5 - <17岁人群中最低;我们的数据过于稀疏,无法确定其最高的人群组。
结论
这些估计表明,每例严重程度相当的秋冬pH1N1大流行浪潮可能导致的死亡人数范围从远低于季节性流感相关死亡人数到略高一些,但对幼儿和非老年成年人影响最大。这些影响估计值取决于对总感染发病率的假设,如果有症状感染发病率更高或向成年人转移、病毒毒力增加或医疗系统压力导致治疗欠佳,死亡人数会更多;如果感染或有症状的比例更低,死亡人数会减少。