Department of Infectious Disease Epidemiology, Robert Koch Institute, DGZ-Ring 1, Berlin 13086, Germany.
BMC Public Health. 2012 Mar 27;12:245. doi: 10.1186/1471-2458-12-245.
Surveillance of severe acute respiratory infections (SARI) in sentinel hospitals is recommended to estimate the burden of severe influenza-cases. Therefore, we monitored patients admitted with respiratory infections (RI) in 9 Berlin hospitals from 7.12.2009 to 12.12.2010 according to different case definitions (CD) and determined the proportion of cases with influenza A(H1N1)pdm09 (pH1N1). We compared the sensitivity and specificity of CD for capturing pandemic pH1N1 cases.
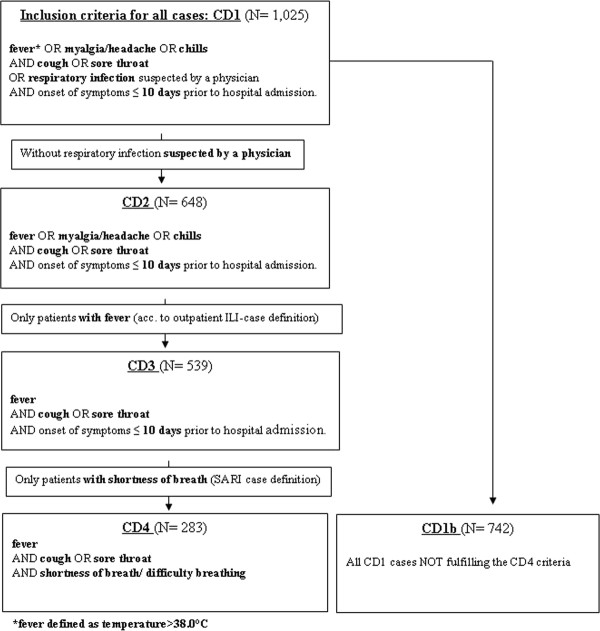
We established an RI-surveillance restricted to adults aged ≤ 65 years within the framework of a pH1N1 vaccine effectiveness study, which required active identification of RI-cases. The hospital information-system was screened daily for newly admitted RI-patients. Nasopharyngeal swabs from consenting patients were tested by PCR for influenza-virus subtypes. Four clinical CD were compared in terms of capturing pH1N1-positives among hospitalized RI-patients by applying sensitivity and specificity analyses. The broadest case definition (CD1) was used for inclusion of RI-cases; the narrowest case definition (CD4) was identical to the SARI case definition recommended by ECDC/WHO.
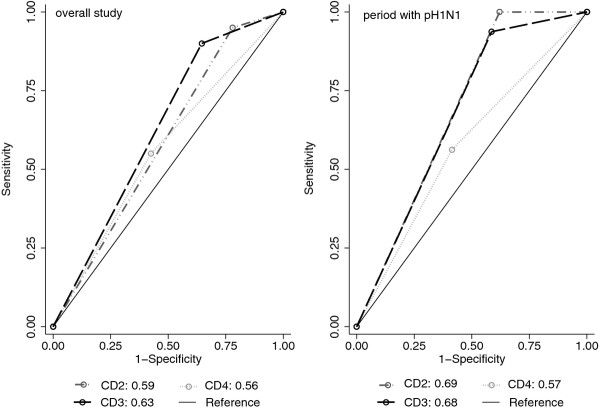
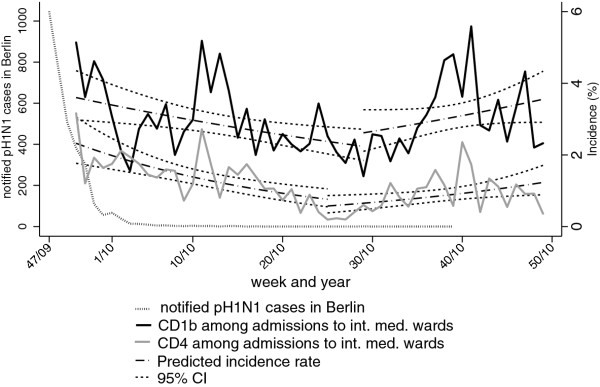
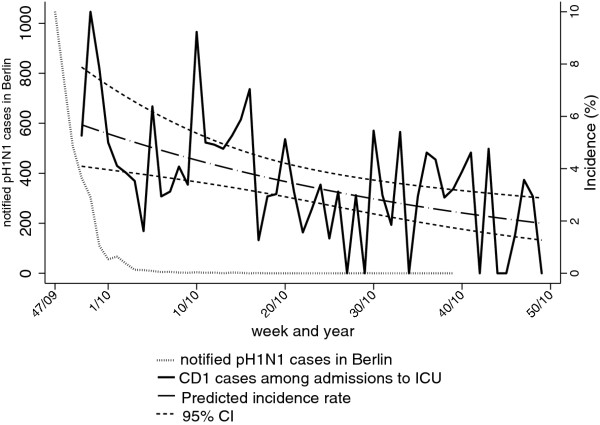
Over the study period, we identified 1,025 RI-cases, of which 283 (28%) met the ECDC/WHO SARI case definition. The percentage of SARI-cases among internal medicine admissions decreased from 3.2% (calendar-week 50-2009) to 0.2% (week 25-2010). Of 354 patients tested by PCR, 20 (6%) were pH1N1-positive. Two case definitions narrower than CD1 but -in contrast to SARI- not requiring shortness of breath yielded the largest areas under the Receiver-Operator-Curve. Heterogeneity of proportions of patients admitted with RI between hospitals was significant.
Comprehensive surveillance of RI cases was feasible in a network of community hospitals. In most settings, several hospitals should be included to ensure representativeness. Although misclassification resulting from failure to obtain symptoms in the hospital information-system cannot be ruled out, a high proportion of hospitalized PCR-positive pH1N1-patients (45%) did not fulfil the SARI case-definition that included shortness of breath or difficulty breathing. Thus, to assess influenza-related disease burden in hospitals, broader, alternative case definitions should be considered.
监测哨点医院严重急性呼吸道感染(SARI),可用于估算严重流感病例的负担。因此,我们根据不同的病例定义(CD),对 2009 年 12 月 7 日至 2010 年 12 月 12 日期间柏林 9 家医院收治的呼吸感染(RI)患者进行监测,并确定甲型 H1N1pdm09(pH1N1)病例的比例。我们比较了这些病例定义捕捉大流行 pH1N1 病例的敏感性和特异性。
我们在 pH1N1 疫苗效力研究的框架内建立了 RI 监测,该研究仅限于年龄≤65 岁的成年人,需要主动识别 RI 病例。医院信息系统每天筛查新入院的 RI 患者。对同意的患者进行鼻咽拭子 PCR 检测流感病毒亚型。通过应用敏感性和特异性分析,比较了四种临床病例定义在捕捉住院 RI 患者 pH1N1 阳性方面的效果。最广泛的病例定义(CD1)用于纳入 RI 病例;最窄的病例定义(CD4)与 ECDC/WHO 推荐的 SARI 病例定义相同。
在研究期间,我们共确定了 1025 例 RI 病例,其中 283 例(28%)符合 ECDC/WHO 的 SARI 病例定义。内科住院患者中 SARI 病例的比例从第 50 周(2009 年)的 3.2%降至第 25 周(2010 年)的 0.2%。354 例接受 PCR 检测的患者中,20 例(6%)为 pH1N1 阳性。两个比 CD1 窄但不需要呼吸急促的病例定义,与 SARI 不同,得到了最大的受试者工作特征曲线下面积。医院间 RI 患者入院比例的异质性具有统计学意义。
在社区医院网络中,对 RI 病例进行全面监测是可行的。在大多数情况下,应纳入多个医院以确保代表性。尽管不能排除因未能在医院信息系统中获取症状而导致的分类错误,但高比例的住院 PCR 阳性 pH1N1 患者(45%)不符合包括呼吸急促或呼吸困难在内的 SARI 病例定义。因此,为了评估医院内流感相关疾病负担,应考虑使用更广泛的替代病例定义。