Department of Diagnostic Radiology, Yonsei University College of Medicine, Seoul, Korea.
Yonsei Med J. 2009 Dec 31;50(6):789-95. doi: 10.3349/ymj.2009.50.6.789. Epub 2009 Dec 18.
The risk of hepatocellular carcinoma (HCC) recurrence must be considered ahead of surgery. This study was undertaken to identify pre-operative risk factors for early intrahepatic recurrence of HCC after curative resection in a large-scale.
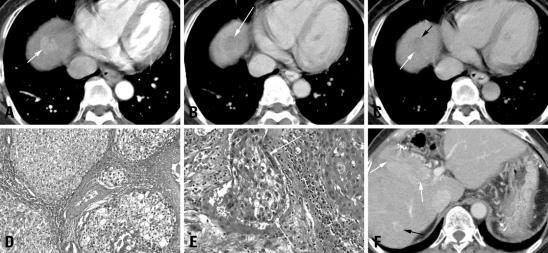
We retrospectively reviewed the preoperative three-phase multi-detector CT (MDCT) and laboratory data for 240 HCC patients who underwent curative resection; tumor size, number, gross shape, capsule integrity, distinctiveness of tumor margin, portal vein thrombosis (PVT), alpha-fetoprotein level (AFP), and protein induced by vitamin K absence-II (PIVKA-II) levels were assessed. Surgical pathology was reviewed; tumor differentiation, capsule, necrosis, and micro-vessel invasion were recorded.
HCC recurred in 61 patients within six months (early recurrence group), but not in 179 patients (control group). In univariate analysis, large tumor size (p = 0.018), shape (p = 0.028), poor capsule integrity (p = 0.046), elevated AFP (p = 0.015), and PIVKA-II (p = 0.008) were significant preoperative risk factors. Among the pathologic features, PVT (p = 0.023), Glisson's capsule penetration (p = 0.033), microvascular invasion (p < 0.001), and poor differentiation (p = 0.001) showed statistical significance. In multivariate analysis, only the histopathologic parameters of microvascular invasion and poor differentiation achieved statistical significance.
Preoperative CT and laboratory parameters showed limited value, while the presence of microscopic vascular tumor invasion and poorly differentiated HCC correlated with higher risk of early recurrence after curative resection.
在手术前必须考虑肝细胞癌(HCC)复发的风险。本研究旨在确定在大规模人群中根治性切除术后 HCC 早期肝内复发的术前危险因素。
我们回顾性分析了 240 例接受根治性切除术的 HCC 患者的术前三期多排 CT(MDCT)和实验室数据;评估肿瘤大小、数量、大体形状、包膜完整性、肿瘤边界清晰度、门静脉血栓形成(PVT)、甲胎蛋白(AFP)和维生素 K 缺乏诱导蛋白 II(PIVKA-II)水平。手术病理检查;记录肿瘤分化、包膜、坏死和微血管侵犯。
61 例患者在 6 个月内(早期复发组)出现 HCC 复发,但 179 例患者(对照组)未复发。单因素分析显示,肿瘤较大(p = 0.018)、形状不规则(p = 0.028)、包膜完整性差(p = 0.046)、AFP 升高(p = 0.015)和 PIVKA-II 升高(p = 0.008)是术前显著的危险因素。在病理特征中,PVT(p = 0.023)、Glisson 包膜穿透(p = 0.033)、微血管侵犯(p < 0.001)和低分化(p = 0.001)具有统计学意义。多因素分析显示,只有微血管侵犯和低分化的组织病理学参数具有统计学意义。
术前 CT 和实验室参数的价值有限,而微血管肿瘤侵犯和低分化 HCC 的存在与根治性切除术后早期复发的风险增加相关。