Tropical Epidemiology Group, Department of Epidemiology and Public Health, London School of Hygiene and Tropical Medicine, London, UK.
Malar J. 2010 Jan 4;9:4. doi: 10.1186/1475-2875-9-4.
Several criteria have been used to assess agreement between replicate slide readings of malaria parasite density. Such criteria may be based on percent difference, or absolute difference, or a combination. Neither the rationale for choosing between these types of criteria, nor that for choosing the magnitude of difference which defines acceptable agreement, are clear. The current paper seeks a procedure which avoids the disadvantages of these current options and whose parameter values are more clearly justified.
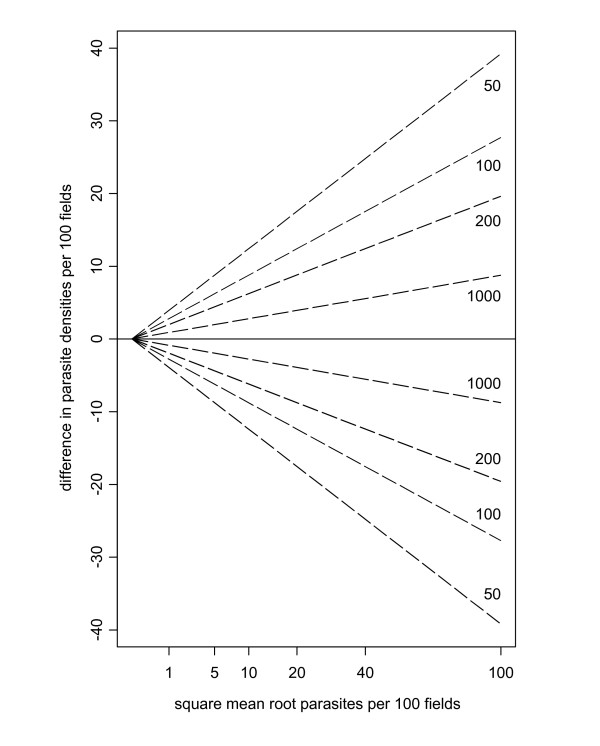
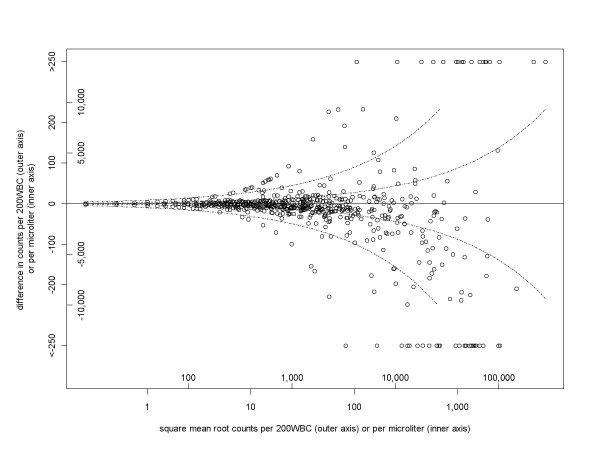
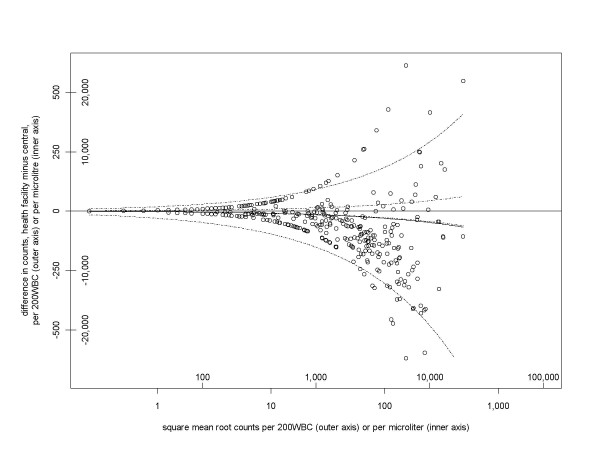
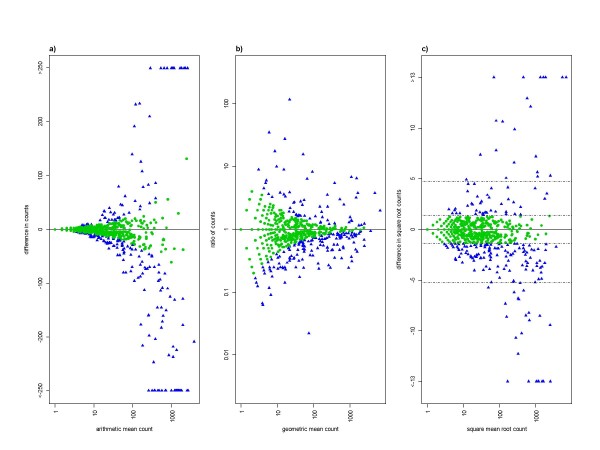
Variation of parasite density within a slide is expected, even when it has been prepared from a homogeneous sample. This places lower limits on sensitivity and observer agreement, quantified by the Poisson distribution. This means that, if a criterion of fixed percent difference criterion is used for satisfactory agreement, the number of discrepant readings is over-estimated at low parasite densities. With a criterion of fixed absolute difference, the same happens at high parasite densities. For an ideal slide, following the Poisson distribution, a criterion based on a constant difference in square root counts would apply for all densities. This can be back-transformed to a difference in absolute counts, which, as expected, gives a wider range of acceptable agreement at higher average densities. In an example dataset from Tanzania, observed differences in square root counts correspond to a 95% limits of agreement of -2,800 and +2,500 parasites/microl at average density of 2,000 parasites/microl, and -6,200 and +5,700 parasites/microl at 10,000 parasites/microl. However, there were more outliers beyond those ranges at higher densities, meaning that actual coverage of these ranges was not a constant 95%, but decreased with density. In a second study, a trial of microscopist training, the corresponding ranges of agreement are wider and asymmetrical: -8,600 to +5,200/microl, and -19,200 to +11,700/microl, respectively. By comparison, the optimal limits of agreement, corresponding to Poisson variation, are +/- 780 and +/- 1,800 parasites/microl, respectively. The focus of this approach on the volume of blood read leads to other conclusions. For example, no matter how large a volume of blood is read, some densities are too low to be reliably detected, which in turn means that disagreements on slide positivity may simply result from within-slide variation, rather than reading errors.
The proposed method defines limits of acceptable agreement in a way which allows for the natural increase in variability with parasite density. This includes defining the levels of between-reader variability, which are consistent with random variation: disagreements within these limits should not trigger additional readings. This approach merits investigation in other settings, in order to determine both the extent of its applicability, and appropriate numerical values for limits of agreement.
已有多种标准用于评估疟疾寄生虫密度的重复玻片阅读结果的一致性。这些标准可能基于百分比差异或绝对差异,或者是两者的组合。但目前尚不清楚选择这些类型的标准的理由,也不清楚选择可接受一致性的差异量的理由。本文旨在寻求一种方法来避免这些现有方法的缺点,并且其参数值更具合理性。
即使从均质样本制备的玻片,其内部的寄生虫密度也会发生变化。这就对敏感性和观察者之间的一致性设置了下限,其下限可以通过泊松分布来量化。这意味着,如果使用固定百分比差异标准来评估满意的一致性,则在寄生虫密度较低时,不一致的读数数量会被高估。如果使用固定绝对差异标准,则在寄生虫密度较高时也会发生这种情况。对于理想的玻片,根据泊松分布,基于平方根计数的恒定差异的标准将适用于所有密度。这可以反向转换为绝对计数的差异,如预期的那样,在较高的平均密度下,可接受的一致性范围更宽。在来自坦桑尼亚的一个示例数据集,观察到的平方根计数差异对应于平均密度为 2000 个寄生虫/微升时的 95%一致性界限为-2800 和+2500 个寄生虫/微升,以及平均密度为 10000 个寄生虫/微升时的-6200 和+5700 个寄生虫/微升。然而,在较高的密度下,超出这些范围的离群值更多,这意味着这些范围的实际覆盖率不是恒定的 95%,而是随着密度的增加而降低。在第二项研究中,对显微镜师培训的试验,相应的一致性范围更宽且不对称:-8600 至+5200/微升,-19200 至+11700/微升,分别。相比之下,对应的最佳一致性界限,对应于泊松分布的变化,分别为 +/-780 和 +/-1800 个寄生虫/微升。该方法将重点放在读取的血量上,会产生其他结论。例如,无论读取多少血量,有些密度太低而无法可靠检测,这反过来意味着在玻片阳性方面的分歧可能只是由于玻片内的变化,而不是读取错误。
本研究提出的方法以允许寄生虫密度自然增加变异性的方式定义可接受的一致性界限。这包括定义与随机变化一致的读者之间差异水平:在这些界限内的分歧不应触发额外的读数。这种方法值得在其他环境中进行研究,以确定其适用性的程度以及一致性界限的适当数值。