School of Social Work, University of Southern California, Los Angeles, California, USA.
Diabetes Care. 2010 Apr;33(4):706-13. doi: 10.2337/dc09-1711. Epub 2010 Jan 22.
To determine whether evidence-based socioculturally adapted collaborative depression care improves receipt of depression care and depression and diabetes outcomes in low-income Hispanic subjects.
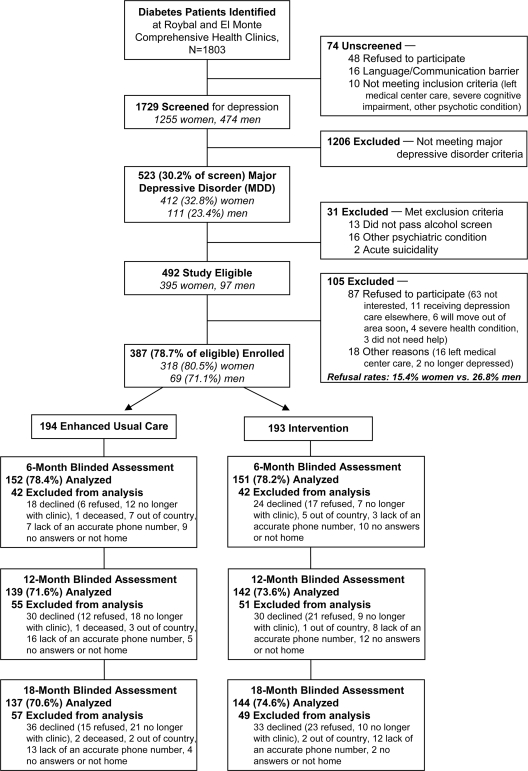
This was a randomized controlled trial of 387 diabetic patients (96.5% Hispanic) with clinically significant depression recruited from two public safety-net clinics from August 2005 to July 2007 and followed over 18 months. Intervention (INT group) included problem-solving therapy and/or antidepressant medication based on a stepped-care algorithm; first-line treatment choice; telephone treatment response, adherence, and relapse prevention follow-up over 12 months; plus systems navigation assistance. Enhanced usual care (EUC group) included standard clinic care plus patient receipt of depression educational pamphlets and a community resource list.
INT patients had significantly greater depression improvement (> or =50% reduction in Symptom Checklist-20 depression score from baseline; 57, 62, and 62% vs. the EUC group's 36, 42, and 44% at 6, 12, and 18 months, respectively; odds ratio 2.46-2.57; P < 0.001). Mixed-effects linear regression models showed a significant study group-by-time interaction over 18 months in diabetes symptoms; anxiety; Medical Outcomes Study Short-Form Health Survey (SF-12) emotional, physical, and pain-related functioning; Sheehan disability; financial situation; and number of social stressors (P = 0.04 for disability and SF-12 physical functioning, P < 0.001 for all others) but no study group-by-time interaction in A1C, diabetes complications, self-care management, or BMI.
Socioculturally adapted collaborative depression care improved depression, functional outcomes, and receipt of depression treatment in predominantly Hispanic patients in safety-net clinics.
确定基于循证的社会文化适应性合作性抑郁护理是否能改善低收入西班牙裔患者接受抑郁护理的情况以及抑郁和糖尿病的结局。
这是一项对 2005 年 8 月至 2007 年 7 月从两家公共医疗保障诊所招募的 387 名有临床显著抑郁症状的糖尿病患者(96.5%为西班牙裔)进行的随机对照试验,随访时间超过 18 个月。干预组(INT 组)包括基于阶梯式护理算法的问题解决治疗和/或抗抑郁药物;一线治疗选择;12 个月内进行电话治疗反应、依从性和复发预防随访;以及系统导航协助。增强型常规护理(EUC 组)包括标准的诊所护理以及患者接受抑郁教育小册子和社区资源清单。
INT 组患者的抑郁改善程度显著更大(从基线开始,症状清单-20 抑郁评分减少≥50%;分别为 6 个月时的 57%、12 个月时的 62%和 18 个月时的 62%,而 EUC 组的分别为 36%、42%和 44%;优势比 2.46-2.57;P < 0.001)。混合效应线性回归模型显示,在 18 个月的时间里,研究组与时间的交互作用在糖尿病症状、焦虑、医疗结果研究短型健康调查问卷(SF-12)的情感、身体和与疼痛相关的功能、Sheehan 残疾、财务状况和社会压力源数量上有显著差异(残疾和 SF-12 身体功能的 P = 0.04,所有其他指标的 P < 0.001),但在 A1C、糖尿病并发症、自我护理管理或 BMI 方面没有研究组与时间的交互作用。
社会文化适应性合作性抑郁护理改善了安全网诊所中以西班牙裔为主的患者的抑郁状况、功能结局以及抑郁治疗的接受程度。