Rajasekaran S, Kamath Vijay, Kiran R, Shetty Ajoy Prasad
Department of Orthopaedics and Spine Surgery, Ganga Hospital, 313, Mettupalayam Road, Coimbatore - 641 011, Tamil Nadu, India.
Indian J Orthop. 2010 Jan;44(1):57-63. doi: 10.4103/0019-5413.58607.
The association of intraspinal neural anomalies with scoliosis is known for more than six decades. However, there are no studies documenting the incidence of association of intraspinal anomalies in scoliotic patients in the Indian population. The guide lines to obtain an magnetic resonance imaging (MRI) scan to rule out neuro-axial abnormalities in presumed adolescent idiopathic scoliosis are also not clear. We conducted a prospective study (a) to document and analyze the incidence and types of intraspinal anomalies in different types of scoliosis in Indian patients. (b) to identify clinico-radiological 'indicators' that best predict the findings of neuro-axial abnormalities in patients with presumed adolescent idiopathic scoliosis, which will alert the physician to the possible presence of intraspinal anomalies and optimize the use of MRI in this sub group of patients.
The data from 177 consecutive scoliotic patients aged less than 21 years were analyzed. Patients were categorized into three groups; Group A - congenital scoliosis (n=60), group B -presumed idiopathic scoliosis (n=94) and group C - scoliosis secondary to neurofibromatosis, neuromuscular and connective tissue disorders (n=23). The presence and type of anomaly in the MRI was correlated to patient symptoms, clinical signs and curve characteristics.
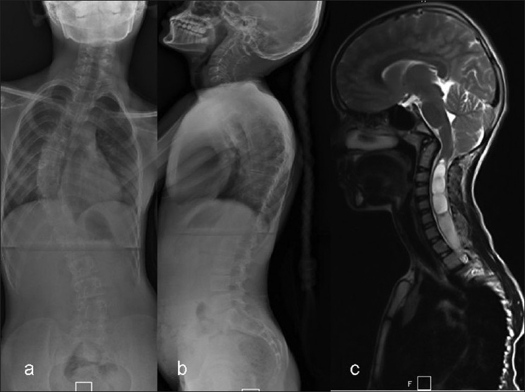
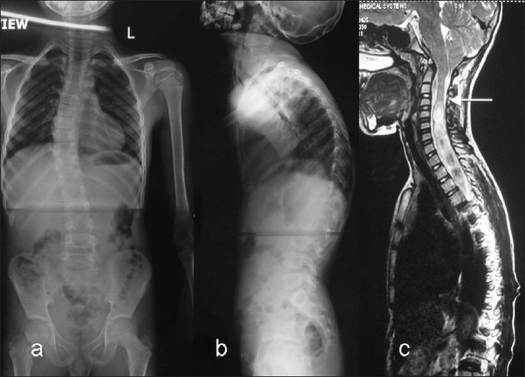
The incidence of intraspinal anomalies in congenital scoliosis was 35% (21/60), with tethered cord due to filum terminale being the commonest anomaly (10/21). Patients with multiple vertebral anomalies had the highest incidence (48%) of neural anomalies and isolated hemi vertebrae had none. In presumed 'idiopathic' scoliosis patients the incidence was higher (16%) than previously reported. Arnold Chiari-I malformation (AC-I) with syringomyelia was the most common neural anomaly (9/15) and the incidence was higher in the presence of neurological findings (100%), apical kyphosis (66.6%) and early onset scoliosis. Isolated lumbar curves had no anomalies. In group-C, incidence was 22% and most of the anomalies were in curves with connective tissue disorders.
The high incidence of intraspinal anomalies in presumed idiopathic scoliosis in our study group emphasizes the need for detailed examination for subtle neurological signs that accompany neuro-axial anomalies. Preoperative MRI screening is recommended in patients with presumed 'idiopathic' scoliosis who present at young age, with neurological findings and in curves with apical thoracic kyphosis.
脊柱内神经异常与脊柱侧弯的关联已被知晓超过60年。然而,尚无研究记录印度人群中脊柱侧弯患者脊柱内异常的关联发生率。对于疑似青少年特发性脊柱侧弯患者,获取磁共振成像(MRI)扫描以排除神经轴异常的指南也不明确。我们进行了一项前瞻性研究:(a)记录和分析印度患者不同类型脊柱侧弯中脊柱内异常的发生率和类型。(b)识别临床放射学“指标”,以最佳预测疑似青少年特发性脊柱侧弯患者的神经轴异常情况,这将提醒医生注意脊柱内异常的可能存在,并优化该亚组患者的MRI使用。
分析了177例年龄小于21岁的连续脊柱侧弯患者的数据。患者分为三组;A组 - 先天性脊柱侧弯(n = 60),B组 - 疑似特发性脊柱侧弯(n = 94),C组 - 神经纤维瘤病、神经肌肉和结缔组织疾病继发的脊柱侧弯(n = 23)。MRI中异常的存在和类型与患者症状、临床体征和曲线特征相关。
先天性脊柱侧弯中脊柱内异常的发生率为35%(21/60),终丝导致的脊髓栓系是最常见的异常(10/21)。有多个椎体异常的患者神经异常发生率最高(48%),孤立半椎体患者无神经异常。在疑似“特发性”脊柱侧弯患者中,发生率高于先前报道(16%)。阿诺德·奇亚里I型畸形(AC-I)伴脊髓空洞症是最常见的神经异常(9/15),在有神经学表现(100%)、顶椎后凸(66.6%)和早发性脊柱侧弯时发生率更高。孤立的腰椎曲线无异常。在C组中,发生率为22%,大多数异常存在于结缔组织疾病相关的曲线中。
我们研究组中疑似特发性脊柱侧弯患者脊柱内异常的高发生率强调了对伴随神经轴异常的细微神经学体征进行详细检查的必要性。对于年轻出现、有神经学表现以及有胸椎顶椎后凸曲线的疑似“特发性”脊柱侧弯患者,建议术前进行MRI筛查。