Department of Neurosurgery, Millard Fillmore Hospital, University at Buffalo, State University of New York, Buffalo, New York, USA.
J Stroke Cerebrovasc Dis. 2010 Mar;19(2):153-62. doi: 10.1016/j.jstrokecerebrovasdis.2010.01.001.
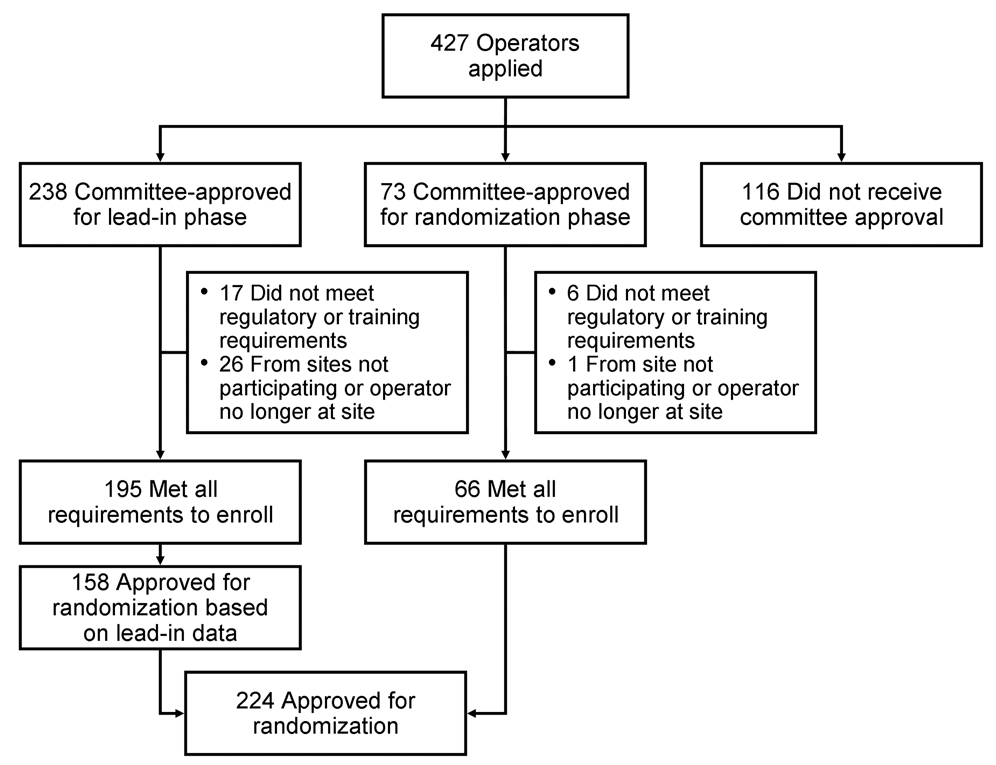
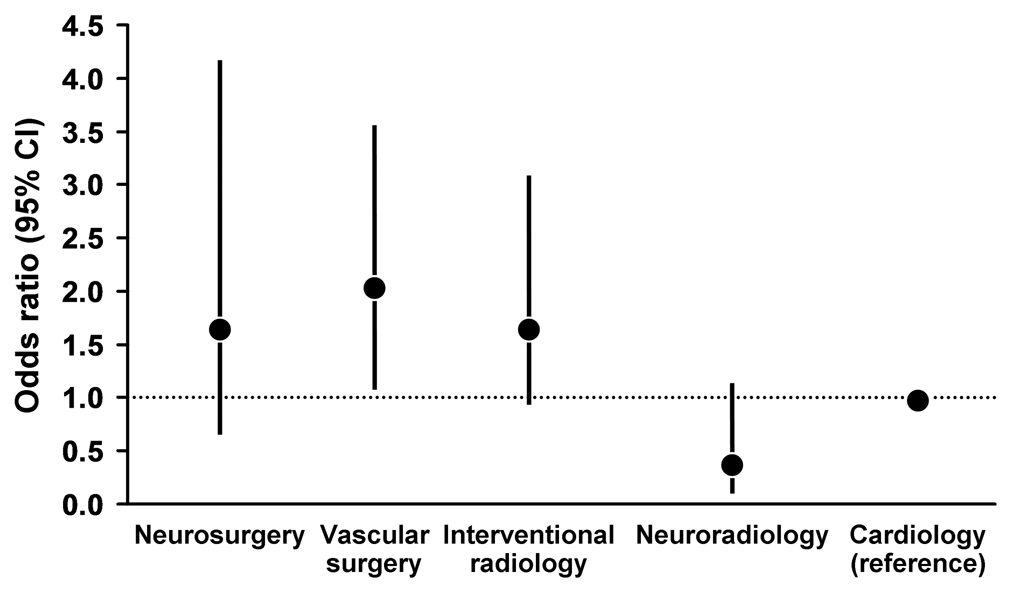
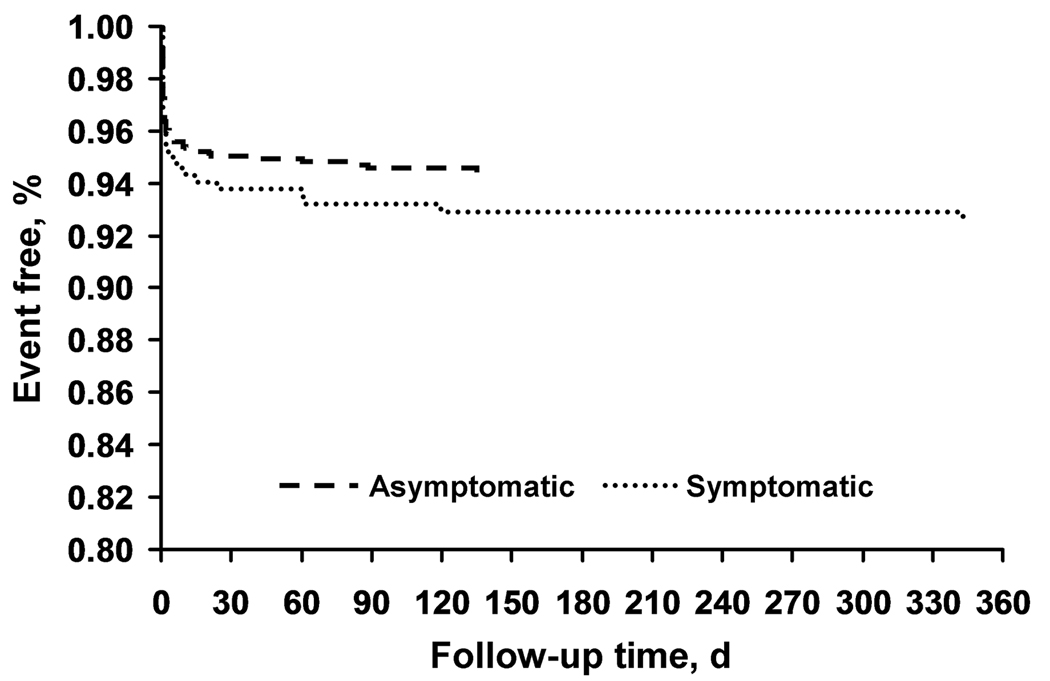
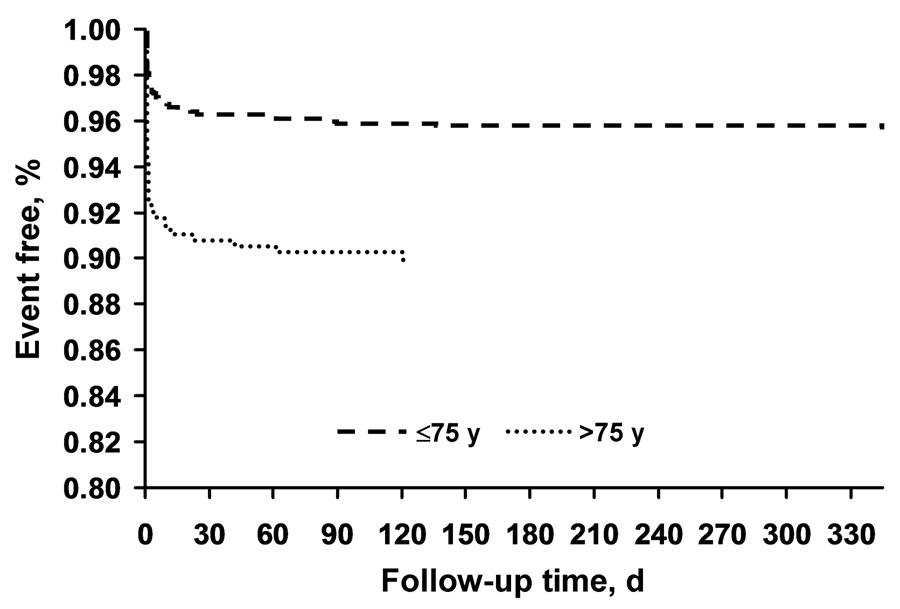
The success of carotid artery stenting in preventing stroke requires a low risk of periprocedural stroke and death. A comprehensive training and credentialing process was prerequisite to the randomized Carotid Revascularization Endarterectomy versus Stenting Trial (CREST) to assemble a competent team of interventionalists with low periprocedural event rates. Interventionalists submitted cases to a multidisciplinary Interventional Management Committee. This committee evaluated 427 applicants. Of these, 238 (56%) were selected to participate in the training program and the lead-in phase, 73 (17%) who had clinical registry experience and satisfactory results with the devices used in CREST were exempt from training and were approved for the randomized phase, and 116 (27%) did not qualify for training. At 30 days in the lead-in study, stroke, myocardial infarction, or death occurred in 6.1% of symptomatic subjects and 4.8% of asymptomatic subjects. Stroke or death occurred in 5.8% of symptomatic subjects and 3.8% of asymptomatic subjects. Outcomes were better for younger subjects and varied by operator training. Based on experience, training, and lead-in results, the Interventional Management Committee selected 224 interventionalists to participate in the randomized phase of CREST. We believe that the credentialing and training of interventionalists participating in CREST have been the most rigorous reported to date for any randomized trial evaluating endovascular treatments. The study identified competent operators, which ensured that the randomized trial results fairly contrasted outcomes between endarterectomy and stenting.
颈动脉支架置入术预防中风的成功需要围手术期中风和死亡的风险低。全面的培训和认证过程是随机颈动脉血管重建内膜切除术与支架置入术试验(CREST)的先决条件,旨在组建一支具有低围手术期事件率的有能力的介入专家团队。介入专家向多学科介入管理委员会提交病例。该委员会评估了 427 名申请者。其中,238 名(56%)被选中参加培训计划和先导阶段,73 名(17%)有临床注册经验,并对 CREST 中使用的器械取得了满意的结果,免于培训,并被批准参加随机阶段,116 名(27%)不符合培训条件。在先导研究的 30 天内,症状性患者中有 6.1%和无症状患者中有 4.8%发生中风、心肌梗死或死亡。症状性患者中有 5.8%和无症状患者中有 3.8%发生中风或死亡。结果对于年轻患者更好,且因操作者的培训而异。根据经验、培训和先导结果,介入管理委员会选择了 224 名介入专家参加 CREST 的随机阶段。我们认为,参与 CREST 的介入专家的认证和培训是迄今为止任何评估血管内治疗的随机试验中最严格的。该研究确定了有能力的操作者,这确保了随机试验结果公平地对比了内膜切除术和支架置入术的结果。