Eide Per K, Brean Are
Department of Neurosurgery, Rikshospitalet University Hospital, Oslo, Norway.
Cerebrospinal Fluid Res. 2010 Feb 12;7:5. doi: 10.1186/1743-8454-7-5.
We have previously seen that idiopathic normal pressure hydrocephalus (iNPH) patients having elevated intracranial pressure (ICP) pulse amplitude consistently respond to shunt surgery. In this study we explored how the cerebrospinal fluid pressure (CSFP) pulse amplitude determined during lumbar infusion testing, correlates with ICP pulse amplitude determined during over-night ICP monitoring and with response to shunt surgery. Our goal was to establish a more reliable screening procedure for selecting iNPH patients for shunt surgery using lumbar intrathecal infusion.
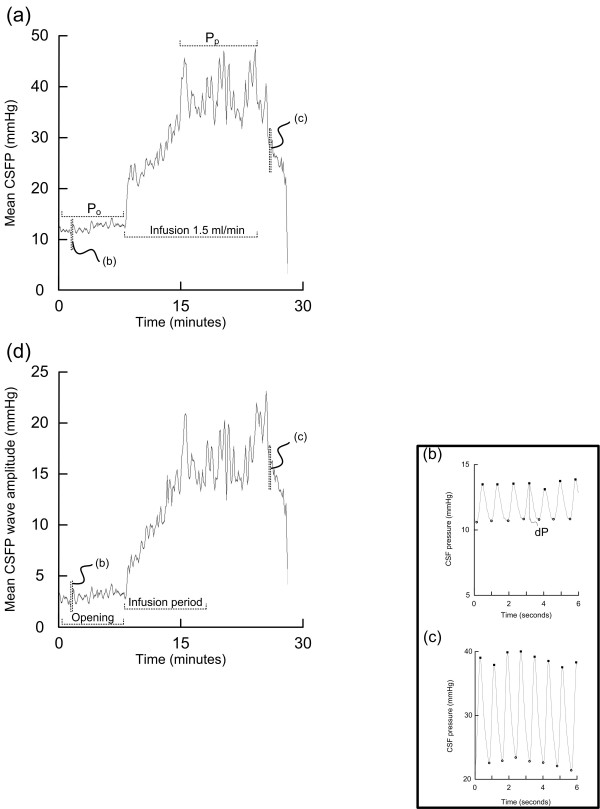
The study population consisted of all iNPH patients undergoing both diagnostic lumbar infusion testing and continuous over-night ICP monitoring during the period 2002-2007. The severity of iNPH was assessed using our NPH grading scale before surgery and 12 months after shunting. The CSFP pulse was characterized from the amplitude of single pressure waves.
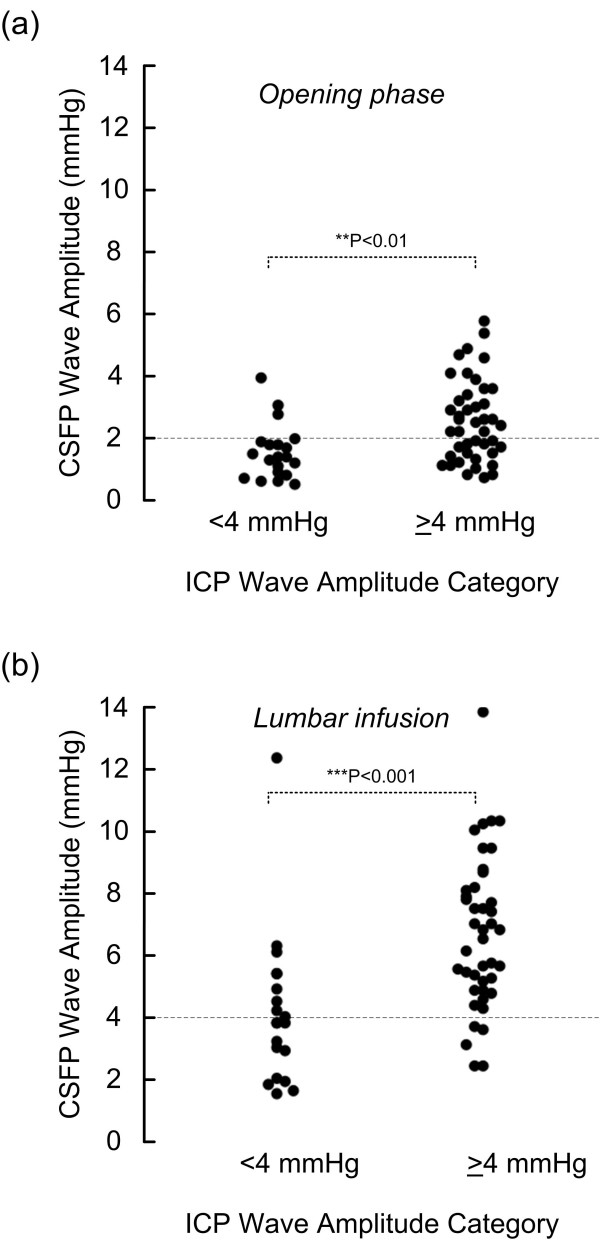
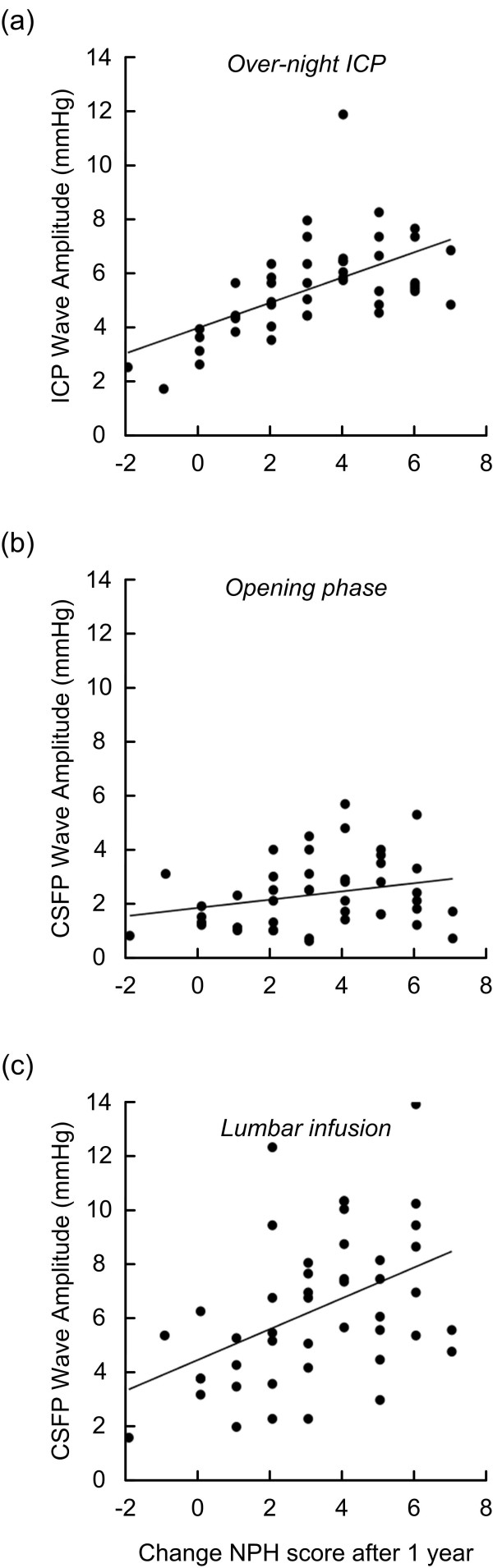
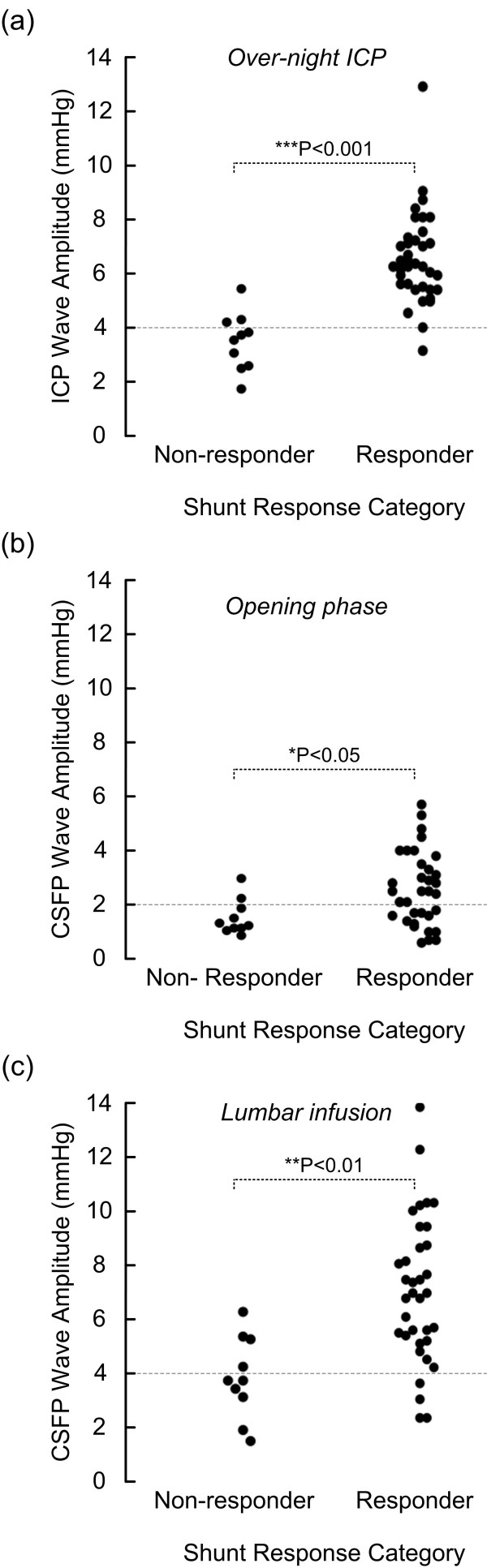
Totally 62 iNPH patients were included, 45 of them underwent shunt surgery, in whom 78% were shunt responders. Among the 45 shunted patients, resistance to CSF outflow (R(out)) was elevated (>or= 12 mmHg/ml/min) in 44. The ICP pulse amplitude recorded over-night was elevated (i.e. mean ICP wave amplitude >or= 4 mmHg) in 68% of patients; 92% of these were shunt responders. In those with elevated overnight ICP pulse amplitude, we found also elevated CSFP pulse amplitude recorded during lumbar infusion testing, both during the opening phase following lumbar puncture and during a standardized period of lumbar infusion (15 ml Ringer over 10 min). The clinical response to shunting after 1 year strongly associated with the over-night ICP pulse amplitude, and also with the pulsatile CSFP during the period of lumbar infusion. Elevated CSFP pulse amplitude during lumbar infusion thus predicted shunt response with sensitivity of 88 and specificity of 60 (positive and negative predictive values of 89 and 60, respectively).
In iNPH patients, shunt response can be anticipated in 9/10 patients with elevated overnight ICP pulse amplitude, while in only 1/10 with low ICP pulse amplitude. Additionally, the CSFP pulse amplitude during lumbar infusion testing was elevated in patients with elevated over-night ICP pulse amplitude. In particular, measurement of CSFP pulse amplitude during a standardized infusion of 15 ml Ringer over 10 min was useful in predicting response to shunt surgery and can be used as a screening procedure for selection of iNPH patients for shunting.
我们之前已经发现,颅内压(ICP)脉搏振幅升高的特发性正常压力脑积水(iNPH)患者对分流手术始终有反应。在本研究中,我们探讨了腰椎灌注测试期间测定的脑脊液压力(CSFP)脉搏振幅与夜间ICP监测期间测定的ICP脉搏振幅以及与分流手术反应之间的相关性。我们的目标是建立一种更可靠的筛查程序,用于通过腰椎鞘内灌注选择适合分流手术的iNPH患者。
研究人群包括2002年至2007年期间接受诊断性腰椎灌注测试和连续夜间ICP监测的所有iNPH患者。在手术前和分流后12个月使用我们的NPH分级量表评估iNPH的严重程度。通过单个压力波的振幅来表征CSFP脉搏。
共纳入62例iNPH患者,其中45例接受了分流手术,其中78%为分流反应者。在45例接受分流手术的患者中,44例脑脊液流出阻力(R(out))升高(≥12 mmHg/ml/min)。夜间记录的ICP脉搏振幅在68%的患者中升高(即平均ICP波振幅≥4 mmHg);其中92%为分流反应者。在夜间ICP脉搏振幅升高的患者中,我们还发现腰椎灌注测试期间记录的CSFP脉搏振幅升高,无论是在腰椎穿刺后的开放期还是在标准化的腰椎灌注期(10分钟内注入15 ml林格液)。1年后分流的临床反应与夜间ICP脉搏振幅密切相关,也与腰椎灌注期间的搏动性CSFP密切相关。因此,腰椎灌注期间CSFP脉搏振幅升高预测分流反应的敏感性为88,特异性为60(阳性和阴性预测值分别为89和60)。
在iNPH患者中,9/10夜间ICP脉搏振幅升高的患者可预期有分流反应,而只有1/10 ICP脉搏振幅低的患者有分流反应。此外,夜间ICP脉搏振幅升高的患者腰椎灌注测试期间的CSFP脉搏振幅升高。特别是,在10分钟内标准化注入15 ml林格液期间测量CSFP脉搏振幅有助于预测分流手术反应,并可作为选择适合分流的iNPH患者的筛查程序。