Department of Medicine, Division of Pulmonary and Critical Care Medicine, University of California San Francisco, San Francisco, CA, USA.
Crit Care Med. 2010 Jun;38(6):1436-41. doi: 10.1097/CCM.0b013e3181de42ad.
Plasma interleukin-8 levels of <220 pg/mL have an excellent negative predictive value (94% to 95%) for death at 28 days in children with septic shock and thus may be useful for risk stratification in clinical trial enrollment in this population. Whether plasma interleukin-8 would have similar utility in adults with septic shock is unknown.
Analysis of plasma interleukin-8 levels and prospectively collected clinical data from patients enrolled in two large randomized controlled trials of ventilator strategy for acute lung injury.
Intensive care units of university hospitals participating in the National Institutes of Health Acute Respiratory Distress Syndrome Network.
One hundred ninety-two adult patients with vasopressor-dependent septic shock.
None.
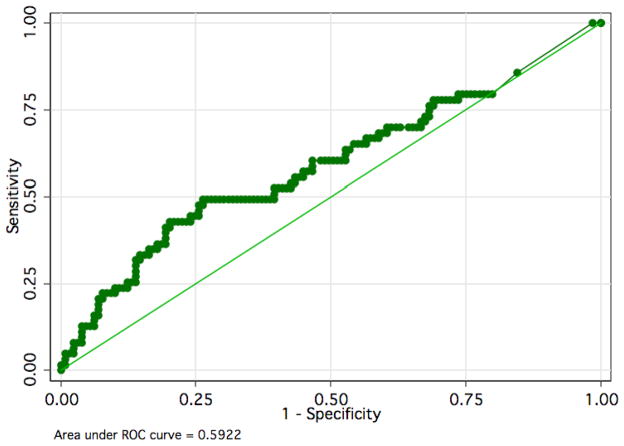
Plasma interleukin-8 levels > or =220 pg/mL were significantly associated with death at 28 days in this cohort (odds ratio, 2.92; 95% confidence interval, 1.42 to 5.99; p = .001). However, in contrast to the findings in pediatric septic shock, a plasma interleukin-8 cutoff <220 pg/mL had a negative predictive value for death of only 74% (95% confidence interval, 66% to 81%) in adults with septic shock. Receiver operating characteristic analysis found an area under the curve of 0.59 for plasma interleukin-8, indicating that plasma interleukin-8 is a poor predictor of mortality in this group. In adults aged <40 yrs, a plasma interleukin-8 cutoff <220 pg/mL had a negative predictive value of 92%.
In contrast to similar pediatric patients, plasma interleukin-8 levels are not an effective risk stratification tool in older adults with septic shock. Future studies of biomarkers for risk stratification in critically ill subjects will need to be replicated in multiple different populations before being applied in screening for clinical trials.
在患有感染性休克的儿童中,血浆白细胞介素-8 水平<220pg/ml 具有极好的阴性预测值(94%至 95%),可用于 28 天死亡的风险分层,因此可能对该人群临床试验的入组有用。在患有感染性休克的成年人中,血浆白细胞介素-8 是否具有类似的作用尚不清楚。
对来自两个大型呼吸机治疗急性肺损伤随机对照试验的患者血浆白细胞介素-8 水平和前瞻性收集的临床数据进行分析。
参与美国国立卫生研究院急性呼吸窘迫综合征网络的大学医院的重症监护病房。
192 例依赖升压药的感染性休克成年患者。
无。
在该队列中,血浆白细胞介素-8 水平>或=220pg/ml 与 28 天死亡显著相关(优势比,2.92;95%置信区间,1.42 至 5.99;p=0.001)。然而,与儿科感染性休克的研究结果相反,在感染性休克患者中,血浆白细胞介素-8 截断值<220pg/ml 的阴性预测值仅为 74%(95%置信区间,66%至 81%)。受试者工作特征曲线分析发现血浆白细胞介素-8 的曲线下面积为 0.59,表明血浆白细胞介素-8 是该组死亡率的一个较差预测因子。在年龄<40 岁的成年人中,血浆白细胞介素-8 截断值<220pg/ml 的阴性预测值为 92%。
与类似的儿科患者不同,在老年感染性休克患者中,血浆白细胞介素-8 水平不是有效的风险分层工具。在对危重患者进行风险分层的生物标志物的进一步研究中,需要在多个不同人群中进行复制,然后才能应用于临床试验的筛选。