Cepkova Magda, Brady Sandra, Sapru Anil, Matthay Michael A, Church Gwynne
The Cardiovascular Research Institute and the Departments of Medicine and Anesthesia, University of California, San Francisco, 505 Parnassus Avenue, M917, San Francisco, CA 94143-0624, USA.
Crit Care. 2006;10(5):R126. doi: 10.1186/cc5037.
Several biological markers of lung injury are predictors of morbidity and mortality in patients with acute lung injury (ALI). The low tidal volume lung-protective ventilation strategy is associated with a significant decrease in plasma biomarker levels compared to the high tidal volume ventilation strategy. The primary objective of this study was to test whether the institution of lung-protective positive pressure ventilation in spontaneously ventilating patients with ALI exacerbates pre-existing lung injury by using measurements of biomarkers of lung injury before and after intubation.
A prospective observational cohort study was conducted in the intensive care unit of a tertiary care university hospital. Twenty-five intubated, mechanically ventilated patients with ALI were enrolled. Physiologic data and serum samples were collected within 6 hours before intubation and at two different time points within the first 24 hours after intubation to measure the concentration of interleukin (IL)-6, IL-8, intercellular adhesion molecule 1 (ICAM-1), and von Willebrand factor (vWF). The differences in biomarker levels before and after intubation were analysed using repeated measures analysis of variance and a paired t test with correction for multiple comparisons.
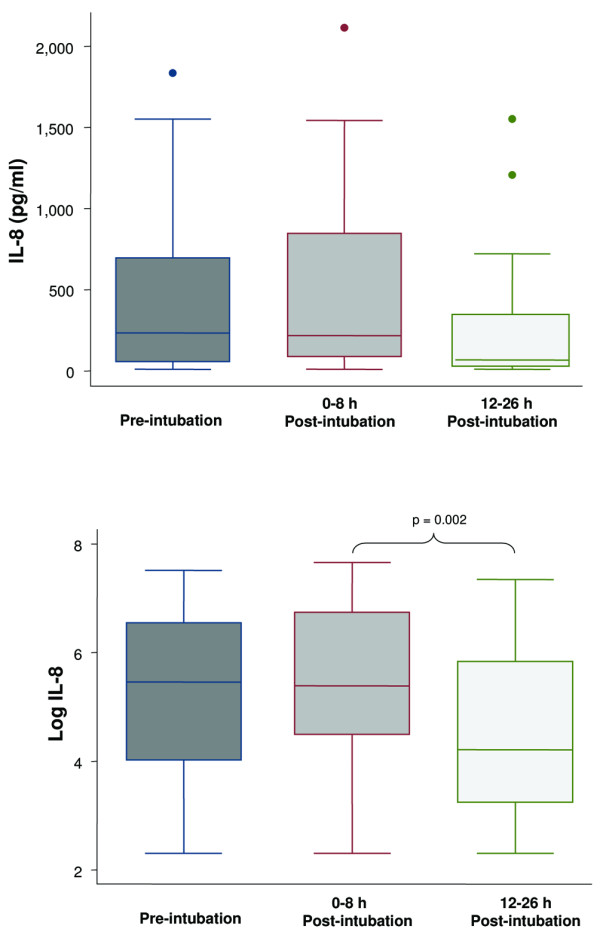
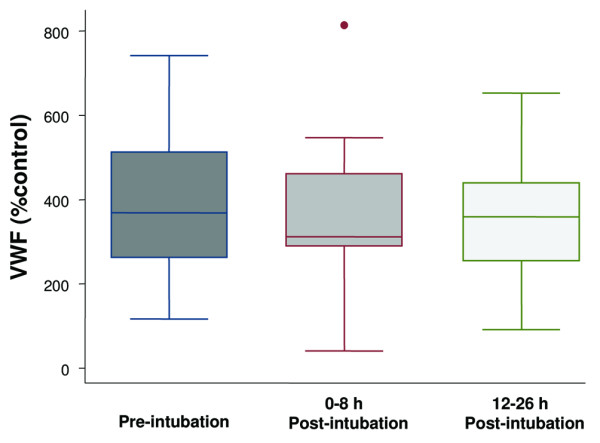
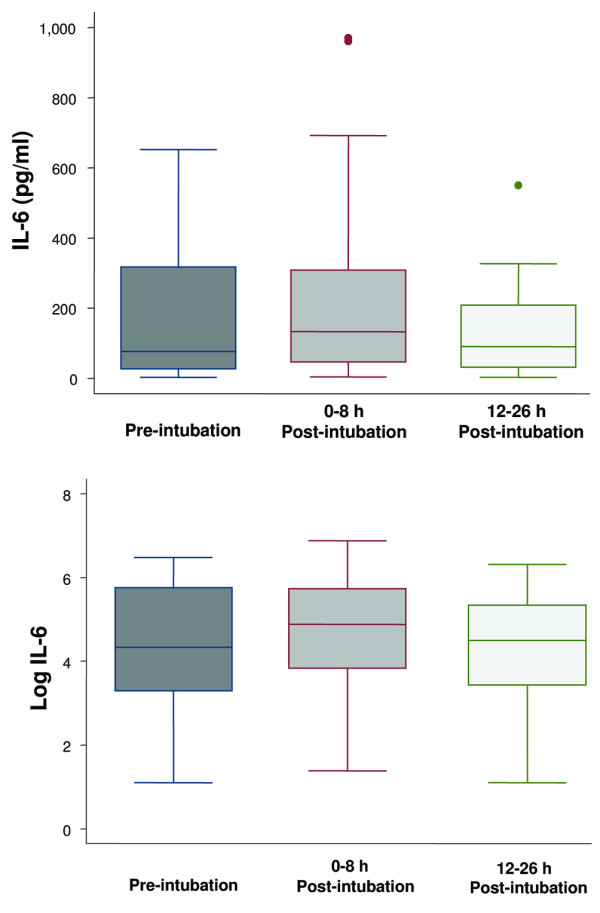
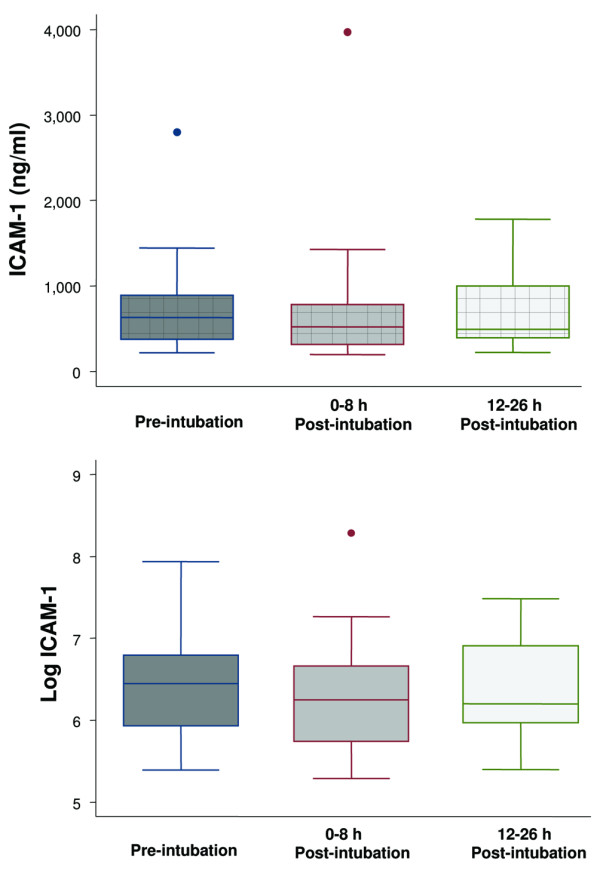
Before endotracheal intubation, all of the biological markers (IL-8, IL-6, ICAM-1, and vWF) were elevated in the spontaneously breathing patients with ALI. After intubation and the institution of positive pressure ventilation (tidal volume 7 to 8 ml/kg per ideal body weight), none of the biological markers was significantly increased at either an early (3 +/- 2 hours) or later (21 +/- 5 hours) time point. However, the levels of IL-8 were significantly decreased at the later time point (21 +/- 5 hours) after intubation. During the 24-hour period after intubation, the PaO2/FiO2 (partial pressure of arterial oxygen/fraction of the inspired oxygen) ratio significantly increased and the plateau airway pressure significantly decreased.
Levels of IL-8, IL-6, vWF, and ICAM-1 are elevated in spontaneously ventilating patients with ALI prior to endotracheal intubation. The institution of a lung-protective ventilation strategy with positive pressure ventilation does not further increase the levels of biological markers of lung injury. The results suggest that the institution of a lung-protective positive pressure ventilation strategy does not worsen the pre-existing lung injury in most patients with ALI.
几种肺损伤生物标志物可预测急性肺损伤(ALI)患者的发病率和死亡率。与高潮气量通气策略相比,低潮气量肺保护性通气策略可使血浆生物标志物水平显著降低。本研究的主要目的是通过测量插管前后肺损伤生物标志物,来检验对自主呼吸的ALI患者实施肺保护性正压通气是否会加重已有的肺损伤。
在一所三级护理大学医院的重症监护病房进行了一项前瞻性观察队列研究。纳入25例经气管插管并接受机械通气的ALI患者。在插管前6小时内以及插管后24小时内的两个不同时间点收集生理数据和血清样本,以测量白细胞介素(IL)-6、IL-8、细胞间黏附分子1(ICAM-1)和血管性血友病因子(vWF)的浓度。使用重复测量方差分析和校正多重比较的配对t检验分析插管前后生物标志物水平的差异。
在气管插管前,所有生物标志物(IL-8、IL-6、ICAM-1和vWF)在自主呼吸的ALI患者中均升高。插管并实施正压通气(潮气量为每理想体重7至8 ml/kg)后,在早期(3±2小时)或晚期(21±5小时)时间点,均无生物标志物显著增加。然而,插管后晚期(21±5小时)IL-8水平显著降低。插管后24小时内,动脉血氧分压/吸入氧分数(PaO2/FiO2)比值显著升高,平台气道压显著降低。
气管插管前,自主呼吸的ALI患者中IL-8、IL-6、vWF和ICAM-1水平升高。实施肺保护性正压通气策略不会进一步增加肺损伤生物标志物水平。结果表明,对大多数ALI患者实施肺保护性正压通气策略不会使已有的肺损伤恶化。