Population Studies and Surveillance, Cancer Care Ontario, 620 University Avenue, Toronto, Ontario, Canada.
Int J Health Geogr. 2010 May 10;9:21. doi: 10.1186/1476-072X-9-21.
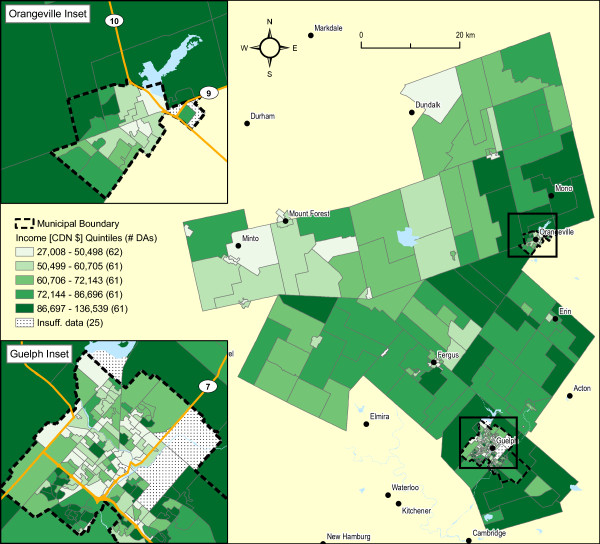
We conducted spatial analyses to determine the geographic variation of cancer at the neighbourhood level (dissemination areas or DAs) within the area of a single Ontario public health unit, Wellington-Dufferin-Guelph, covering a population of 238,326 inhabitants. Cancer incidence data between 1999 and 2003 were obtained from the Ontario Cancer Registry and were geocoded down to the level of DA using the enhanced Postal Code Conversion File. The 2001 Census of Canada provided information on the size and age-sex structure of the population at the DA level, in addition to information about selected census covariates, such as average neighbourhood income.
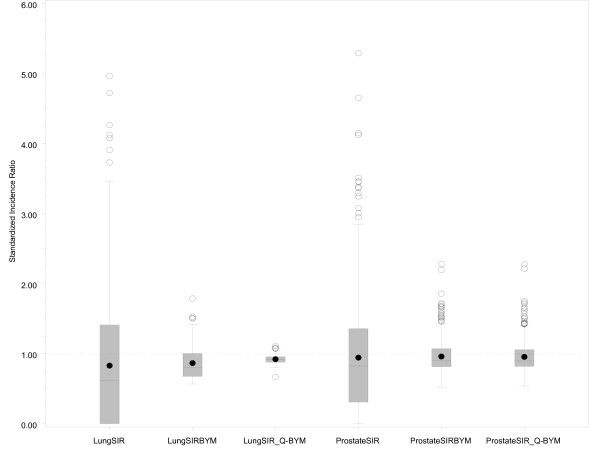
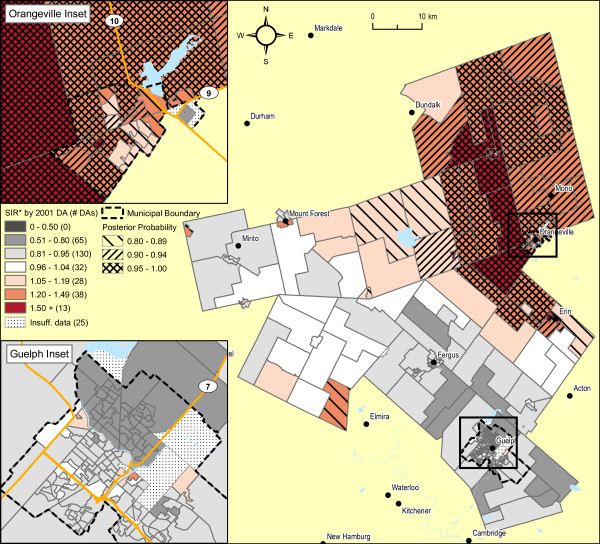
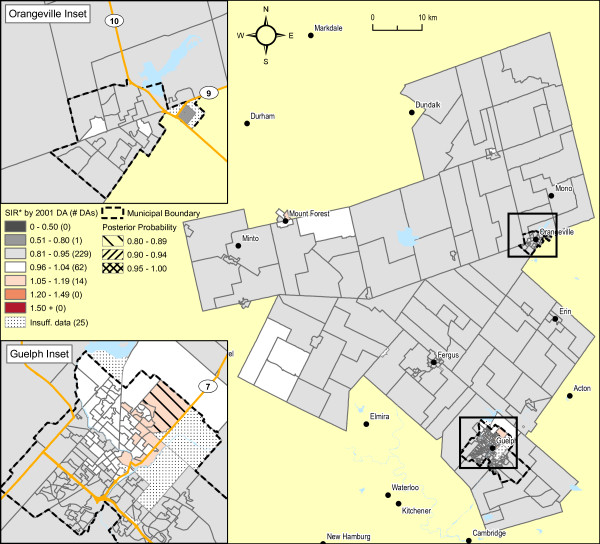
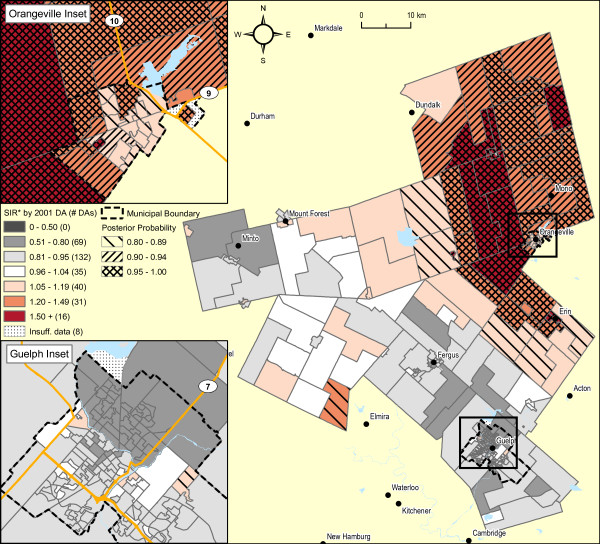
Age standardized incidence ratios for cancer and the prevalence of census covariates were calculated for each of 331 dissemination areas in Wellington-Dufferin-Guelph. The standardized incidence ratios (SIR) for cancer varied dramatically across the dissemination areas. However, application of the Moran's I statistic, a popular index of spatial autocorrelation, suggested significant spatial patterns for only two cancers, lung and prostate, both in males (p < 0.001 and p = 0.002, respectively). Employing Bayesian hierarchical models, areas in the urban core of the City of Guelph had significantly higher SIRs for male lung cancer than the remainder of Wellington-Dufferin-Guelph; and, neighbourhoods in the urban and surrounding rural areas of Orangeville exhibited significantly higher SIRs for prostate cancer. After adjustment for age and spatial dependence, average household income attenuated much of the spatial pattern of lung cancer, but not of prostate cancer.
This paper demonstrates the feasibility and utility of a systematic approach to identifying neighbourhoods, within the area served by a public health unit, that have significantly higher risks of cancer. This exploratory, ecologic study suggests several hypotheses for these spatial patterns that warrant further investigations. To the best of our knowledge, this is the first Canadian study published in the peer-reviewed literature estimating the risk of relatively rare public health outcomes at a very small areal level, namely dissemination areas.
我们进行了空间分析,以确定安大略省单一公共卫生部门辖区内的邻里层面(传播区域或 DA)的癌症地理变异情况,该辖区覆盖了 238326 名居民。1999 年至 2003 年的癌症发病率数据来自安大略癌症登记处,并使用增强型邮政编码转换文件将其地理编码到 DA 级别。2001 年加拿大人口普查提供了 DA 级别的人口规模和年龄性别结构信息,以及有关选定人口普查协变量的信息,例如平均邻里收入。
计算了惠灵顿-达福-吉尔福德 331 个传播区域中每个区域的癌症年龄标准化发病率比和普查协变量的患病率。传播区域的癌症标准化发病率比差异很大。然而,莫兰 I 统计量(一种流行的空间自相关指标)的应用表明,只有两种癌症(男性肺癌和前列腺癌)存在显著的空间模式(分别为 p < 0.001 和 p = 0.002)。使用贝叶斯层次模型,圭尔夫市市区的区域男性肺癌的 SIR 明显高于惠灵顿-达福-吉尔福德的其余地区;而橙镇市区和周边农村地区的社区前列腺癌的 SIR 明显较高。在调整年龄和空间依赖性后,家庭平均收入减弱了肺癌的大部分空间模式,但对前列腺癌没有影响。
本文展示了一种系统方法识别公共卫生部门服务区域内癌症风险显著较高的邻里的可行性和实用性。这项探索性的生态研究提出了一些关于这些空间模式的假设,这些假设值得进一步研究。据我们所知,这是在同行评审文献中发表的第一项估计非常小区域(即传播区域)相对罕见公共卫生结果风险的加拿大研究。