Department of Orthopaedic Surgery, Medical University Innsbruck, Anichstr 35, 6020 Innsbruck, Austria.
Eur Spine J. 2010 Sep;19(9):1415-22. doi: 10.1007/s00586-010-1398-6. Epub 2010 Jun 1.
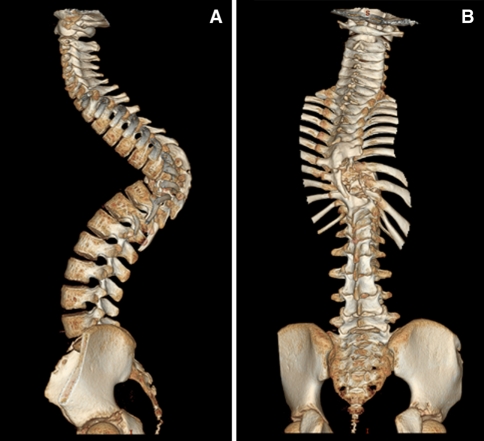
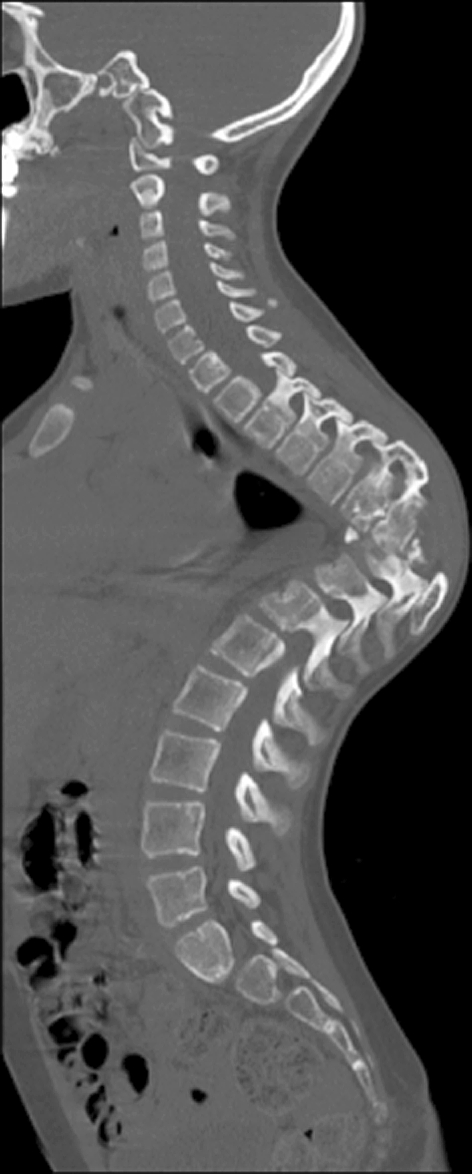
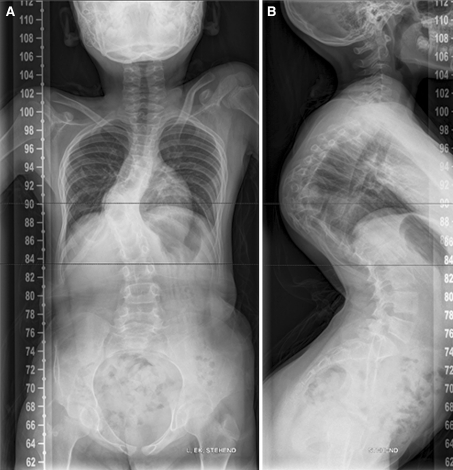
A primary Echinococcus granulosus infection of the spine involving the vertebrae T8 and T9 of a 6-year-old child was treated elsewhere by thoracotomy, partial corporectomy, multiple laminectomies and uninstrumented fusion. Owing to inappropriate stabilization, severe deformity developed secondary to these surgeries. X-rays, CT and MRI scans of the spine revealed a severe thoracic kyphoscoliosis of more than 100 degrees (Fig. 1) and recurrence of Echinococcus granulosus infection. The intraspinal cyst formation was located between the stretched dural sac and the vertebral bodies of the kyphotic apex causing significant compression of the cord (Figs. 2, 3, 4). A progressive neurologic deficit was reported by the patient. At the time of referral, the patient was wheelchair bound and unable to walk by herself (Frankel Grade C). Standard antiinfectious therapy of Echinococcus granulosus requires a minimum treatment period of 3 months. This should be done before any surgical intervention because in case of a rupture of an active cyst, the delivered lipoprotein antigens of the parasite may cause a potentially lethal anaphylactic shock. Owing to the critical neurological status, we decided to perform surgery without full length preoperative antiinfectious therapy. Surgical treatment consisted in posterior vertebral column resection technique with an extensive bilateral costotransversectomy over three levels, re-decompression with cyst excision around the apex and multilevel corporectomy of the apex of the deformity. Stabilisation and correction of the spinal deformity were done by insertion of a vertebral body replacement cage anteriorly and posterior shortening by compression and by a multisegmental pedicle screw construct. After the surgery, antihelminthic therapy was continued. The patients neurological deficits resolved quickly: 4 weeks after surgery, the patient had Frankel Grade D and was ambulatory without any assistance. After an 18-month follow-up, the patient is free of recurrence of infection and free of neurologically deficits (Frankel E). This case demonstrates that inappropriate treatment--partial resection of the cyst, inappropriate anterior stabilization and posterior multilevel laminectomies without posterior stabilization--may lead to severe progressive kyphoscoliotic deformity and recurrence of infection, both leading to significant neurological injury presenting as a very difficult to treat pathology. Fig. 1 X-rays of the patient showing a kyhoscoliotic deformity. a ap view, b lateral view Fig. 2 CT reconstruction of the whole spine showing the apex of the deformity is located in the area of the previous surgeries Fig. 3 Sagittal CT-cut showing the bone bloc at the apex with a translation deformity Fig. 4 Sagittal T2-weighted MRI image showing the cystic formation at the apex.
患者为 6 岁儿童,因原发性细粒棘球蚴感染 T8、T9 胸椎,在外院行剖胸术、部分椎体切除术、多次椎板切除术和非器械融合术治疗。由于固定不当,这些手术后严重畸形。脊柱 X 线、CT 和 MRI 扫描显示严重的胸腰椎后凸畸形超过 100 度(图 1),且细粒棘球蚴感染复发。椎管内囊肿形成于伸展的硬脊膜囊和脊柱后凸顶点的椎体之间,导致脊髓明显受压(图 2、3、4)。患者报告有进行性神经功能缺损。转诊时,患者坐轮椅,无法自行行走(Frankel 分级 C)。细粒棘球蚴的标准抗感染治疗需要至少 3 个月的治疗期。这应在任何手术干预之前进行,因为在活性囊肿破裂的情况下,寄生虫释放的脂蛋白抗原可能会引起潜在致命的过敏性休克。由于神经功能严重受损,我们决定在没有充分术前抗感染治疗的情况下进行手术。手术治疗包括后路脊柱全长切除术,广泛双侧肋横突切除术 3 个节段,在顶点处切除囊肿减压,在畸形顶点进行多节段椎体切除术。通过前路插入椎体置换笼和后路压缩进行脊柱畸形的稳定和矫正,并通过多节段椎弓根螺钉结构进行后缩短。手术后继续进行驱虫治疗。患者的神经功能缺损迅速恢复:术后 4 周,患者的 Frankel 分级为 D,可独立行走,无需任何帮助。18 个月随访时,患者无感染复发,无神经功能缺损(Frankel E)。该病例表明,不适当的治疗——囊肿部分切除、前方固定不当和后路多节段椎板切除术而无后路固定——可能导致严重的进行性后凸侧凸畸形和感染复发,均导致严重的神经损伤,表现为非常难以治疗的病理。
图 1 患者的 X 射线显示后凸侧凸畸形。a 前后位,b 侧位
图 2 全脊柱 CT 重建显示畸形顶点位于先前手术部位
图 3 矢状位 CT 切片显示顶点处的骨块有平移变形
图 4 矢状位 T2 加权 MRI 图像显示顶点处的囊性形成