Division of Endocrinology, Diabetes, Metabolism and Nutrition, Mayo Clinic College of Medicine, Rochester, Minnesota, USA.
Diabetes. 2010 Nov;59(11):2697-707. doi: 10.2337/db10-1032. Epub 2010 Aug 12.
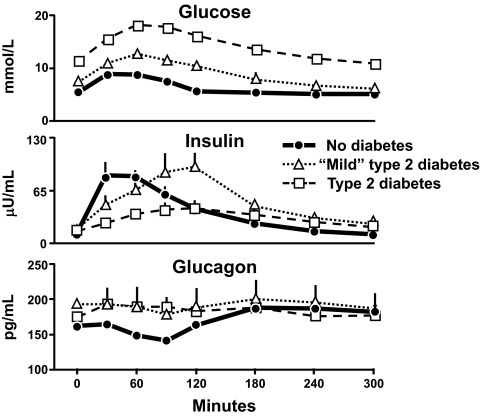
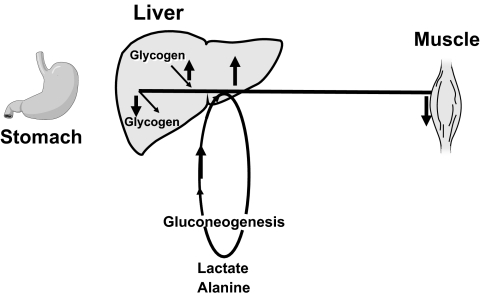
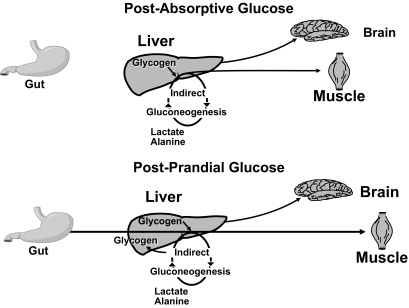
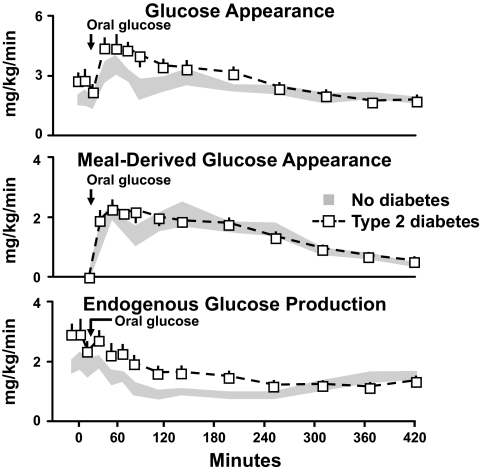
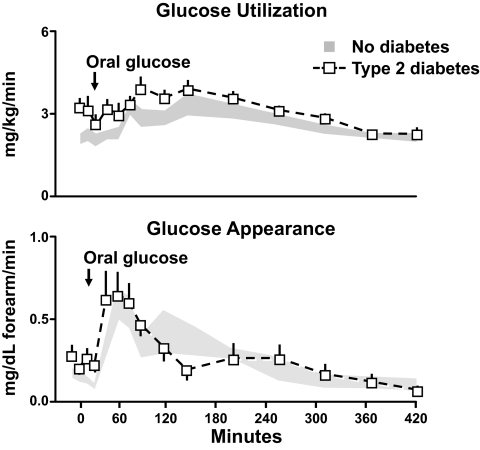
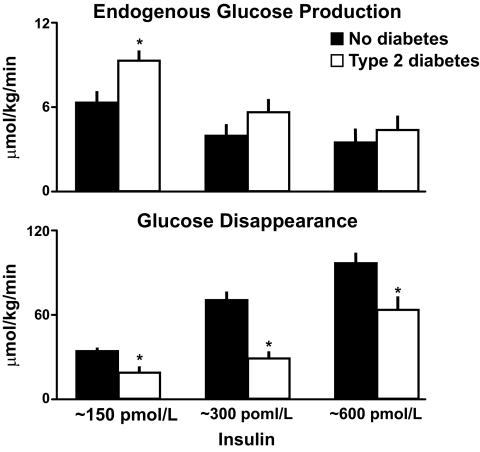
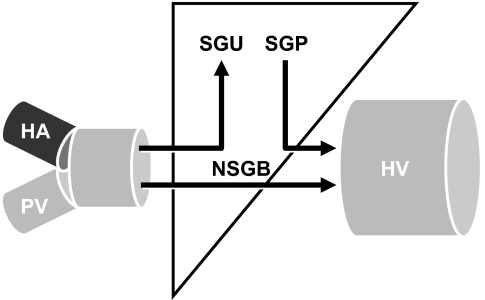
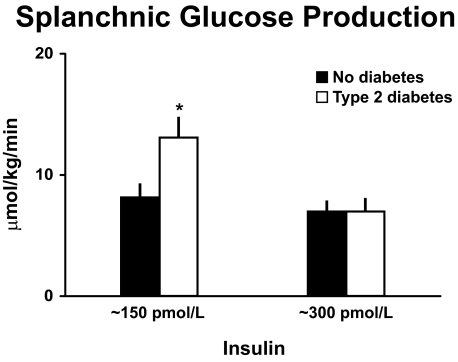
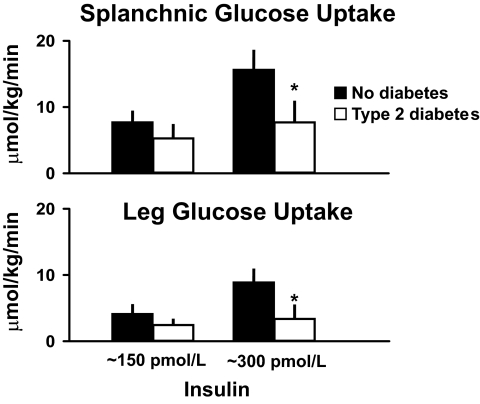
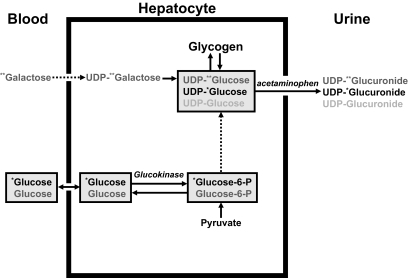
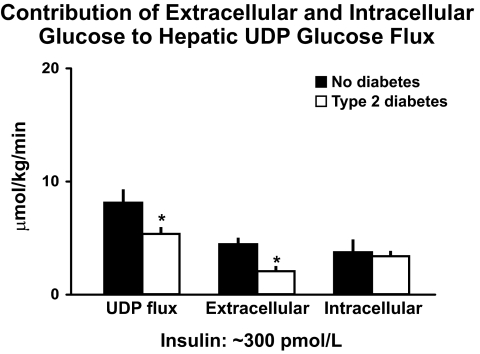
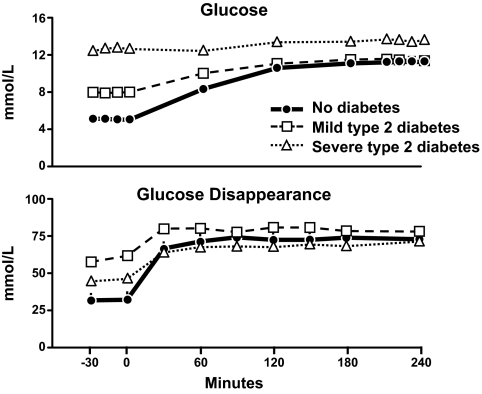
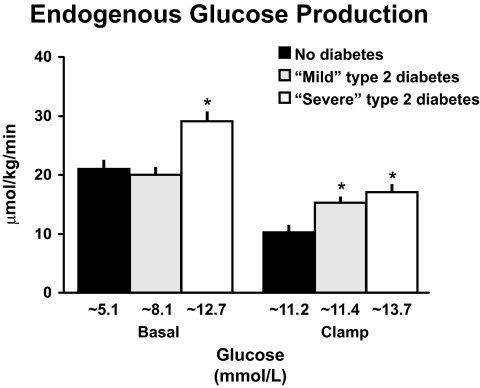
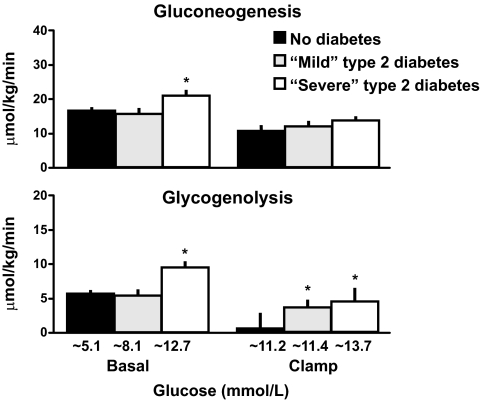
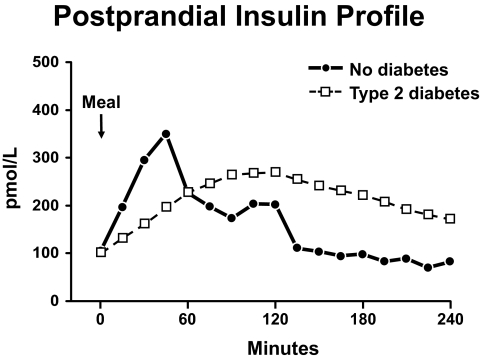
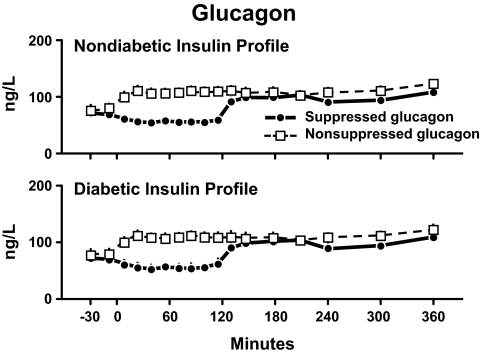
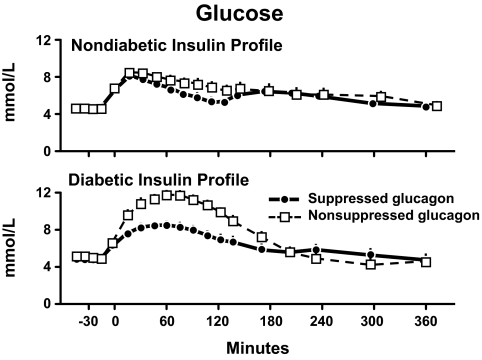
The objective of this research is to gain a greater understanding of the cause of fasting and postprandial hyperglycemia in people with type 2 diabetes. Endogenous glucose production is excessive before eating and fails to appropriately suppress after eating in people with type 2 diabetes. This is due in part to impaired insulin-induced suppression of endogenous glucose production, which is observed early in the evolution of type 2 diabetes. Increased rates of gluconeogenesis and perhaps glycogenolysis contribute to hepatic insulin resistance. Insulin-induced stimulation of hepatic glucose uptake and hepatic glycogen synthesis are reduced in people with type 2 diabetes primarily due to decreased uptake of extracellular glucose presumably because of inadequate activation of hepatic glucokinase. Delayed insulin secretion results in higher peak glucose concentrations particularly when suppression of glucagon is impaired, whereas insulin resistance prolongs the duration of hyperglycemia, which can be marked when both hepatic and extra-hepatic insulin resistance are present. The premise of these studies, as well as those performed by many other investigators, is that an understanding of the pathogenesis of type 2 diabetes will enable the development of targeted therapies that are directed toward correcting specific metabolic defects in a given individual. I, as well as many other investigators, believe that such therapies are likely to be more effective and to have a lower risk than would occur if everyone were treated the same regardless of the underlying cause of their hyperglycemia. While we do not yet have sufficient knowledge to truly individualize therapy, in my opinion this approach will be the norm in the not too distant future.
本研究旨在深入了解 2 型糖尿病患者空腹和餐后高血糖的原因。2 型糖尿病患者在进食前内源性葡萄糖生成过多,进食后无法适当抑制。这部分是由于胰岛素诱导的内源性葡萄糖生成抑制受损,这在 2 型糖尿病的早期演变中就已经观察到。糖异生率增加,可能糖原分解增加,导致肝胰岛素抵抗。2 型糖尿病患者的胰岛素诱导肝葡萄糖摄取和肝糖原合成减少,主要是由于细胞外葡萄糖摄取减少,推测是由于肝葡萄糖激酶激活不足。胰岛素分泌延迟导致血糖峰值升高,尤其是当胰高血糖素抑制受损时,而胰岛素抵抗延长了高血糖的持续时间,如果肝内和肝外胰岛素抵抗同时存在,则可能会出现明显的高血糖。这些研究以及许多其他研究人员的研究前提是,对 2 型糖尿病发病机制的理解将能够开发出针对特定个体纠正特定代谢缺陷的靶向治疗方法。我和许多其他研究人员一样,认为这种治疗方法可能比不分青红皂白地对所有人进行治疗(无论其高血糖的根本原因是什么)更有效,风险更低。虽然我们还没有足够的知识来真正实现个体化治疗,但在我看来,这种方法将在不久的将来成为常态。