Gupta Vivek, Yadav Kapil, Anand K
Centre for Community Medicine, All India Institute of Medical Sciences, New Delhi.
Indian J Community Med. 2010 Apr;35(2):245-51. doi: 10.4103/0970-0218.66877.
Tobacco is the leading cause of mortality globally and in India. The magnitude and the pattern of tobacco consumption are likely to be influenced by the geographical setting and with rapid urbanization in India there is a need to study this differential pattern.
The aim was to study the rural, urban, and urban-slum differences in patterns of tobacco use.
The study was conducted in Ballabgarh block, Faridabad district, Haryana, and was a community-based cross-sectional study.
The study was conducted in years 2003-2004 using the WHO STEPS approach with 7891 participants, approximately equal number of males and females, selected using multistage sampling from urban, urban-slum, and rural strata.
The analysis was done using the SPSS 12.0 statistical package (SPSS Inc., Chicago, IL, USA). Direct standardization to the WHO world standard population was done to and chi-square and ANOVA tests were used for comparison across three study settings.
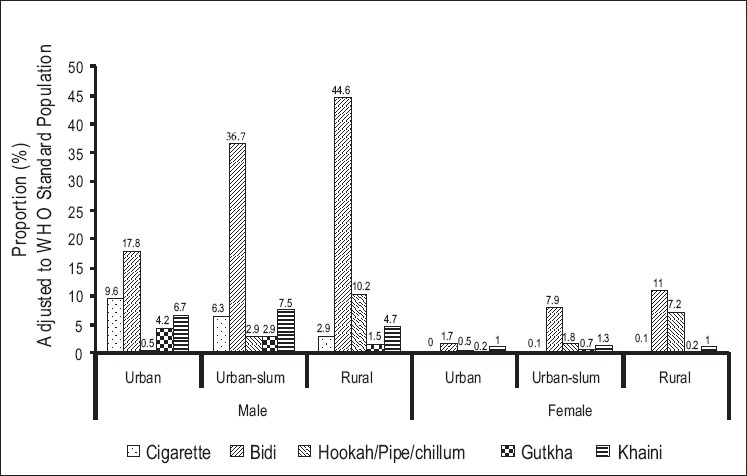
Self-reported tobacco use among males was as follows: urban 35.2%; urban-slums 48.3%; and rural 52.6% (P value <0.05). Self-reported tobacco use among females was as follows: Urban 3.5%; urban-slums 11.9%; and rural 17.7% (P value <0.05). More males reported daily bidi (tobacco wrapped in temburini leaf) smoking (urban 17.8%, urban-slums 36.7%, rural 44.6%) than cigarette use (urban 9.6%, urban-slums 6.3%, rural 2.9%). Females using smoked tobacco were almost exclusively using bidis (urban 1.7%, 7.9%, 11% in rural). Daily chewed tobacco use had urban, urban-slum, and rural gradients of 12%, 10.5%, and 6.8% in males respectively. Its use was low in females.
The antitobacco policies of India need to focus on bidis in antitobacco campaigns. The program activities must find ways to reach the rural and urban-slum populations.
烟草是全球及印度死亡的主要原因。烟草消费的规模和模式可能受地理环境影响,随着印度城市化进程的加快,有必要研究这种差异模式。
研究农村、城市和城市贫民窟在烟草使用模式上的差异。
该研究在哈里亚纳邦法里达巴德区巴拉加尔街区进行,是一项基于社区的横断面研究。
该研究于2003 - 2004年采用世界卫生组织的“逐步调查”方法进行,共有7891名参与者,男女数量大致相等,通过多阶段抽样从城市、城市贫民窟和农村阶层中选取。
使用SPSS 12.0统计软件包(美国伊利诺伊州芝加哥市SPSS公司)进行分析。对世界卫生组织的世界标准人口进行直接标准化,并使用卡方检验和方差分析在三种研究环境中进行比较。
男性自我报告的烟草使用率如下:城市为35.2%;城市贫民窟为48.3%;农村为52.6%(P值<0.05)。女性自我报告的烟草使用率如下:城市为3.5%;城市贫民窟为11.9%;农村为17.7%(P值<0.05)。报告每天吸比迪烟(用坦布里尼叶包裹的烟草)的男性(城市为17.8%,城市贫民窟为36.7%,农村为44.6%)多于吸香烟的男性(城市为9.6%,城市贫民窟为6.3%,农村为2.9%)。使用烟熏烟草的女性几乎都吸比迪烟(城市为1.7%,农村为7.9%,农村为11%)。男性每天嚼烟草的使用率在城市、城市贫民窟和农村分别为12%、10.5%和6.8%。女性的使用率较低。
印度的反烟草政策在反烟草运动中需要关注比迪烟。项目活动必须找到接触农村和城市贫民窟人群的方法。