Department of Internal Medicine and Geriatrics, Academic Medical Center, Room F4-108, PO, Box 22660, 1100 DD Amsterdam, The Netherlands.
BMC Health Serv Res. 2010 Oct 29;10:296. doi: 10.1186/1472-6963-10-296.
Older patients are at high risk for poor outcomes after acute hospital admission. The mortality rate in these patients is approximately 20%, whereas 30% of the survivors decline in their level of activities of daily living (ADL) functioning three months after hospital discharge. Most diseases and geriatric conditions that contribute to poor outcomes could be subject to pro-active intervention; not only during hospitalization, but also after discharge. This paper presents the design of a randomised controlled clinical trial concerning the effect of a pro-active, multi-component, nurse-led transitional care program following patients for six months after hospital admission.
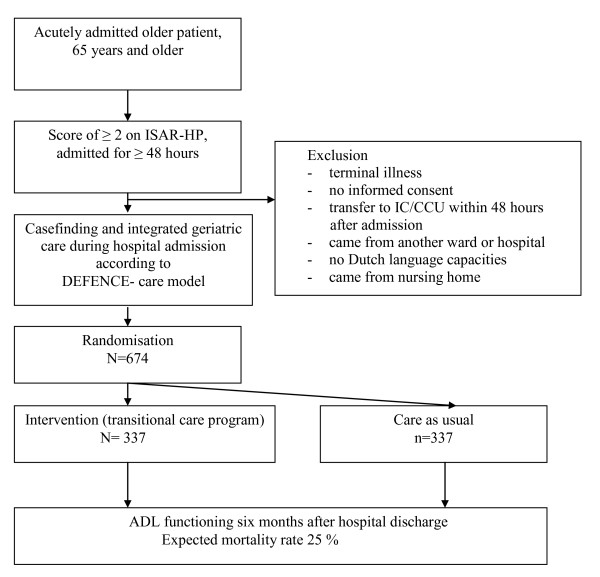
METHODS/DESIGN: Three hospitals in the Netherlands will participate in the multi-centre, double-blind, randomised clinical trial comparing a pro-active multi-component nurse-led transitional care program to usual care after discharge. All patients acutely admitted to the Department of Internal Medicine who are 65 years and older, hospitalised for at least 48 hours and are at risk for functional decline are invited to participate in the study. All patients will receive integrated geriatric care by a geriatric consultation team during hospital admission. Randomization, which will be stratified by study site and cognitive impairment, will be conducted during admission. The intervention group will receive the transitional care bridge program, consisting of a handover moment with a community care Care Nurse (CN) during hospital admission and five home visits after discharge. The control group will receive 'care as usual' after discharge. The main outcome is the level of ADL functioning six months after discharge compared to premorbid functioning measured with the Katz ADL index. Secondary outcomes include; survival, cognitive functioning, quality of life, and health care utilization, satisfaction of the patient and primary care giver with the transitional care bridge program. All outcomes will be measured at three, six and twelve months after discharge. Approximately 674 patients will be enrolled to either the intervention or control group.
The study will provide new knowledge on a combined intervention of integrated care during hospital admission, a proactive handover moment before discharge and intensive home visits after discharge.
NTR 2384.
老年患者在急性住院后出现不良结局的风险较高。这些患者的死亡率约为 20%,而 30%的幸存者在出院后三个月内日常生活活动(ADL)功能下降。导致不良结局的大多数疾病和老年疾病都可以进行积极干预;不仅在住院期间,而且在出院后也可以进行。本文介绍了一项随机对照临床试验的设计,该试验涉及在患者出院后六个月内对积极的、多组分、护士主导的过渡性护理计划的效果。
方法/设计:荷兰的三家医院将参与这项多中心、双盲、随机临床试验,比较积极的多组分护士主导的过渡性护理计划与出院后的常规护理。所有 65 岁及以上、急性住院至少 48 小时且有功能下降风险的内科患者都将被邀请参加这项研究。所有患者在住院期间将接受老年病会诊小组提供的综合老年护理。在住院期间,将根据研究地点和认知障碍进行分层随机化。干预组将接受过渡护理桥接计划,包括在住院期间与社区护理护士(CN)进行交接时刻和出院后进行五次家访。对照组将在出院后接受“常规护理”。主要结局是与发病前的 Katz ADL 指数相比,出院后 6 个月的 ADL 功能水平。次要结局包括:生存、认知功能、生活质量、卫生保健利用、患者和初级保健提供者对过渡护理桥接计划的满意度。所有结局都将在出院后 3、6 和 12 个月进行测量。大约 674 名患者将被分配到干预组或对照组。
该研究将提供关于在住院期间进行综合护理、在出院前积极交接时刻和出院后强化家访相结合的综合干预的新知识。
NTR 2384。