Division of Infectious Diseases, San Martino University Hospital, L,go R, Benzi, 10, Genoa, Italy.
Crit Care. 2010;14(6):R222. doi: 10.1186/cc9365. Epub 2010 Dec 8.
Timely diagnosis of invasive candidiasis (IC) remains difficult as the clinical presentation is not specific and blood cultures lack sensitivity and need a long incubation time. Thus, non-culture-based methods for diagnosing IC have been developed. Mannan antigen (Mn) and anti-mannan antibodies (A-Mn) are present in patients with IC. On behalf of the Third European Conference on Infections in Leukemia, the performance of these tests was analysed and reviewed.
The literature was searched for studies using the commercially available sandwich enzyme-linked immunosorbent assays (Platelia™, Bio-Rad Laboratories, Marnes-la-Coquette, France) for detecting Mn and A-Mn in serum. The target condition of this review was IC defined according to 2008 European Organization for Research and Treatment of Cancer/Mycoses Study Group criteria. Sensitivity, specificity and diagnostic odds ratios (DOR) were calculated for Mn, A-Mn and combined Mn/A-Mn testing.
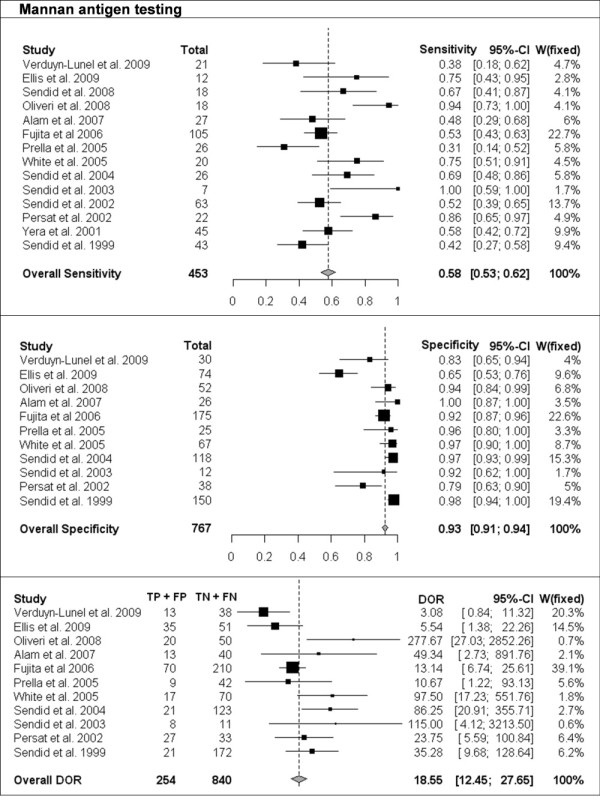
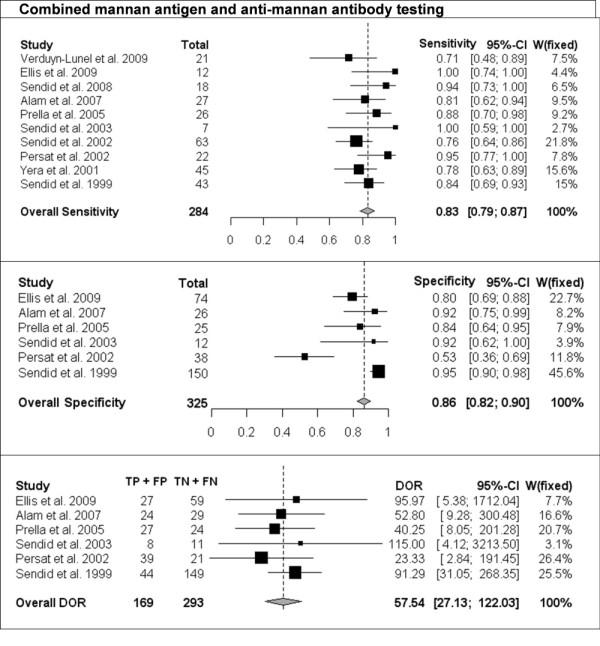
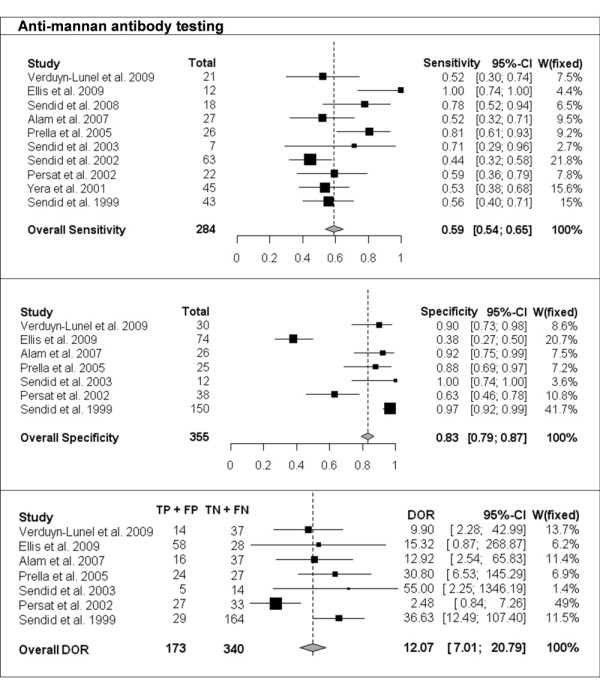
Overall, 14 studies that comprised 453 patients and 767 controls were reviewed. The patient populations included in the studies were mainly haematological and cancer cases in seven studies and mainly intensive care unit and surgery cases in the other seven studies. All studies but one were retrospective in design. Mn sensitivity was 58% (95% confidence interval [CI], 53-62); specificity, 93% (95% CI, 91-94) and DOR, 18 (95% CI 12-28). A-Mn sensitivity was 59% (95% CI, 54-65); specificity, 83% (95% CI, 79-97) and DOR, 12 (95% CI 7-21). Combined Mn/A-Mn sensitivity was 83% (95% CI, 79-87); specificity, 86% (95% CI, 82-90) and DOR, 58 (95% CI 27-122). Significant heterogeneity of the studies was detected. The sensitivity of both Mn and A-Mn varied for different Candida species, and it was the highest for C. albicans, followed by C. glabrata and C. tropicalis. In 73% of 45 patients with candidemia, at least one of the serological tests was positive before the culture results, with mean time advantage being 6 days for Mn and 7 days for A-Mn. In 21 patients with hepatosplenic IC, 18 (86%) had Mn or A-Mn positive test results at a median of 16 days before radiological detection of liver or spleen lesions.
Mn and A-Mn are useful for diagnosis of IC. The performance of combined Mn/A-Mn testing is superior to either Mn or A-Mn testing.
及时诊断侵袭性念珠菌病(IC)仍然具有挑战性,因为临床表现不具特异性,血液培养缺乏敏感性且需要较长的孵育时间。因此,已经开发出了用于诊断 IC 的非培养方法。甘露聚糖抗原(Mn)和抗甘露聚糖抗体(A-Mn)存在于患有 IC 的患者中。代表第三届欧洲白血病感染会议,分析和审查了这些测试的性能。
检索了使用商业上可用的夹心酶联免疫吸附试验(Platelia ™,Bio-Rad Laboratories,Marnes-la-Coquette,法国)检测血清中 Mn 和 A-Mn 的研究。本综述的目标条件是根据 2008 年欧洲癌症研究与治疗组织/真菌病研究组标准定义的 IC。计算了 Mn、A-Mn 和 Mn/A-Mn 联合检测的敏感性、特异性和诊断比值比(DOR)。
总共审查了 14 项研究,这些研究共包括 453 名患者和 767 名对照。研究中的患者人群主要包括 7 项研究中的血液学和癌症病例,以及另外 7 项研究中的重症监护室和手术病例。除一项研究外,所有研究均为回顾性设计。Mn 的敏感性为 58%(95%CI,53-62);特异性为 93%(95%CI,91-94),DOR 为 18(95%CI,12-28)。A-Mn 的敏感性为 59%(95%CI,54-65);特异性为 83%(95%CI,79-97),DOR 为 12(95%CI,7-21)。Mn/A-Mn 联合检测的敏感性为 83%(95%CI,79-87);特异性为 86%(95%CI,82-90),DOR 为 58(95%CI,27-122)。检测到研究之间存在明显的异质性。Mn 和 A-Mn 的敏感性因不同的念珠菌物种而异,对于白色念珠菌,其敏感性最高,其次是光滑念珠菌和热带念珠菌。在 45 名菌血症患者中,有 73%的患者至少有一种血清学检测在培养结果之前呈阳性,Mn 的平均时间优势为 6 天,A-Mn 的平均时间优势为 7 天。在 21 名肝脾 IC 患者中,18 名(86%)在放射学检测到肝脏或脾脏病变之前,Mn 或 A-Mn 检测结果呈阳性,中位时间为 16 天。
Mn 和 A-Mn 可用于诊断 IC。Mn/A-Mn 联合检测的性能优于 Mn 或 A-Mn 检测。