Institut Pasteur-Cambodia, Phnom Penh, Cambodia.
PLoS Negl Trop Dis. 2010 Nov 30;4(11):e903. doi: 10.1371/journal.pntd.0000903.
Dengue vaccines are now in late-stage development, and evaluation and robust estimates of dengue disease burden are needed to facilitate further development and introduction. In Cambodia, the national dengue case-definition only allows reporting of children less than 16 years of age, and little is known about dengue burden in rural areas and among older persons. To estimate the true burden of dengue in the largest province of Cambodia, Kampong Cham, we conducted community-based active dengue fever surveillance among the 0-to-19-year age group in rural villages and urban areas during 2006-2008.
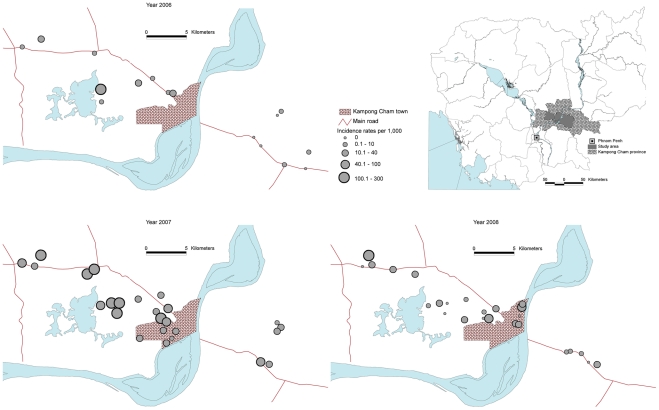
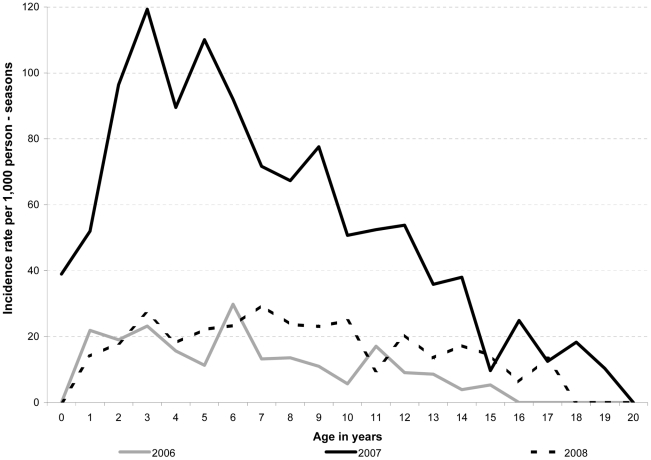
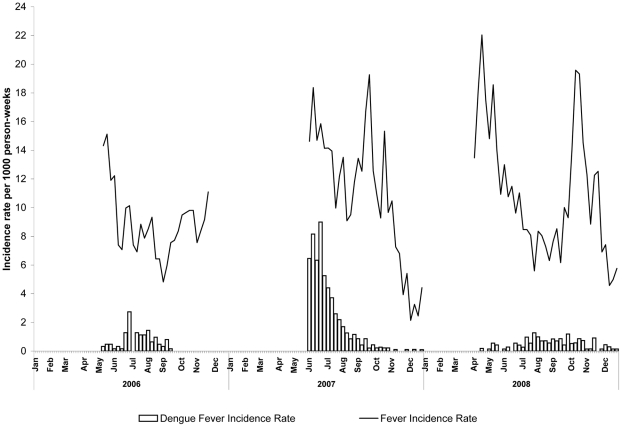
Active surveillance for febrile illness was conducted in 32 villages and 10 urban areas by mothers trained to use digital thermometers combined with weekly home visits to identify persons with fever. An investigation team visited families with febrile persons to obtain informed consent for participation in the follow-up study, which included collection of personal data and blood specimens. Dengue-related febrile illness was defined using molecular and serological testing of paired acute and convalescent blood samples. Over the three years of surveillance, 6,121 fever episodes were identified with 736 laboratory-confirmed dengue virus (DENV) infections for incidences of 13.4-57.8/1,000 person-seasons. Average incidence was highest among children less than 7 years of age (41.1/1,000 person-seasons) and lowest among the 16-to-19-year age group (11.3/1,000 person-seasons). The distribution of dengue was highly focal, with incidence rates in villages and urban areas ranging from 1.5-211.5/1,000 person-seasons (median 36.5). During a DENV-3 outbreak in 2007, rural areas were affected more than urban areas (incidence 71 vs. 17/1,000 person-seasons, p<0.001).
The large-scale active surveillance study for dengue fever in Cambodia found a higher disease incidence than reported to the national surveillance system, particularly in preschool children and that disease incidence was high in both rural and urban areas. It also confirmed the previously observed focal nature of dengue virus transmission.
登革热疫苗目前处于研发后期,为了促进其进一步开发和应用,需要对登革热疾病负担进行评估和准确估算。在柬埔寨,国家登革热病例定义仅允许报告 16 岁以下儿童的病例,而对于农村地区和老年人的登革热负担知之甚少。为了估计柬埔寨最大省份磅湛省的真实登革热负担,我们在 2006 年至 2008 年期间对 0 至 19 岁的农村和城市社区人群进行了基于社区的主动登革热监测。
通过培训母亲使用数字体温计并每周进行家访,对 32 个农村村庄和 10 个城市地区进行了发热性疾病的主动监测,以识别发热者。调查小组访问有发热者的家庭,以获得参与随访研究的知情同意,该研究包括收集个人数据和血液样本。使用分子和血清学检测对配对的急性期和恢复期血液样本进行登革热相关发热性疾病的诊断。在三年的监测期间,共发现 6121 例发热病例,其中 736 例经实验室确认为登革热病毒(DENV)感染,发病率为 13.4-57.8/1000 人季。发病率最高的是 7 岁以下儿童(41.1/1000 人季),发病率最低的是 16-19 岁年龄组(11.3/1000 人季)。登革热的分布高度集中,村庄和城市地区的发病率范围为 1.5-211.5/1000 人季(中位数为 36.5)。在 2007 年的 DENV-3 暴发期间,农村地区的发病率高于城市地区(发病率分别为 71 例和 17 例/1000 人季,p<0.001)。
柬埔寨进行的大规模登革热主动监测研究发现,疾病发病率高于国家监测系统报告的发病率,尤其是学龄前儿童,且农村和城市地区的发病率均较高。该研究还证实了以前观察到的登革热病毒传播的集中性。