National Forensic Mental Health Service, Central Mental Hospital, Dundrum, Dublin 14, Ireland.
BMC Psychiatry. 2011 Mar 16;11:43. doi: 10.1186/1471-244X-11-43.
The assessment of those presenting to prison in-reach and court diversion services and those referred for admission to mental health services is a triage decision, allocating the patient to the appropriate level of therapeutic security. This is a critical clinical decision. We set out to improve on unstructured clinical judgement. We collated qualitative information and devised an 11 item structured professional judgment instrument for this purpose then tested for validity.
All those assessed following screening over a three month period at a busy remand committals prison (n = 246) were rated in a retrospective cohort design blind to outcome. Similarly, all those admitted to a mental health service from the same prison in-reach service over an overlapping two year period were rated blind to outcome (n = 100).
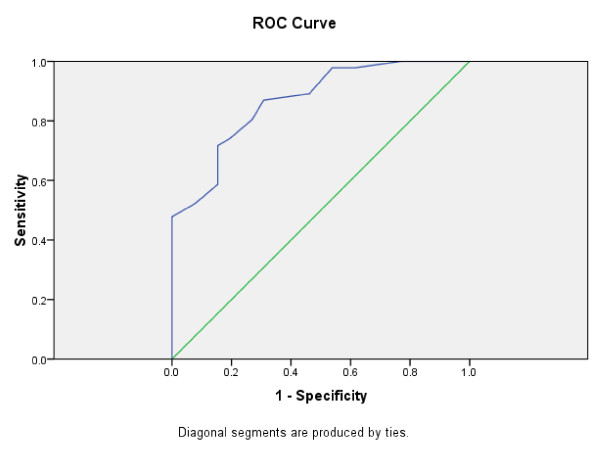
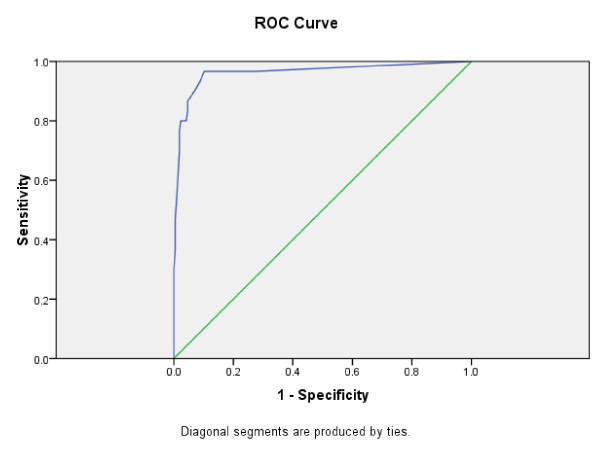
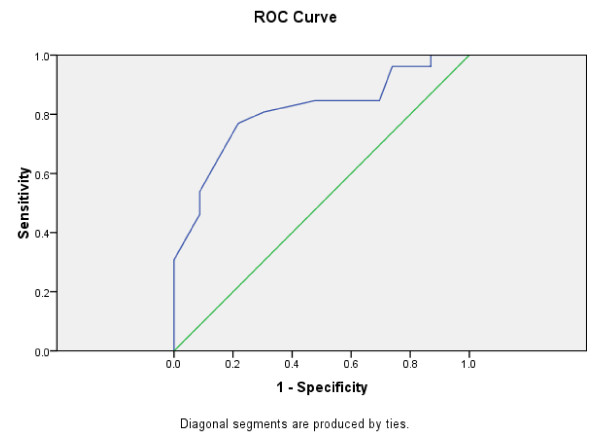
The 11 item scale had good internal consistency (Cronbach's alpha = 0.95) and inter-rater reliability. The scale score did not correlate with the HCR-20 'historical' score. For the three month sample, the receiver operating characteristic area under the curve (AUC) for those admitted to hospital was 0.893 (95% confidence interval 0.843 to 0.943). For the two year sample, AUC distinguished at each level between those admitted to open wards, low secure units or a medium/high secure service. Open wards v low secure units AUC = 0.805 (95% CI 0.680 to 0.930); low secure v medium/high secure AUC = 0.866, (95% CI 0.784 to 0.949). Item to outcome correlations were significant for all 11 items.
The DUNDRUM-1 triage security scale and its items performed to criterion levels when tested against the real world outcome. This instrument can be used to ensure consistency in decision making when deciding who to admit to secure forensic hospitals. It can also be used to benchmark admission thresholds between services and jurisdictions. In this study we found some divergence between assessed need and actual placement. This provides fertile ground for future research as well as practical assistance in assessing unmet need, auditing case mix and planning care pathways.
对监狱内入所和法庭分流服务中出现的患者以及转介到精神卫生服务机构的患者进行评估是一种分诊决策,将患者分配到适当的治疗安全级别。这是一个关键的临床决策。我们旨在改善非结构化临床判断。为此,我们收集了定性信息,并为此设计了一个 11 项的结构化专业判断工具,然后对其进行了有效性测试。
在一个繁忙的还押监狱进行三个月的筛查后,对所有接受评估的患者(n=246)进行回顾性队列设计,对其进行盲法评估。同样,在重叠的两年期间,对同一监狱内入所服务中被转介到精神卫生服务机构的所有患者(n=100)进行盲法评估。
该 11 项量表具有良好的内部一致性(Cronbach's alpha=0.95)和评分者间信度。该量表评分与 HCR-20“历史”评分不相关。对于三个月的样本,被收入医院的患者的接受者操作特征曲线下面积(AUC)为 0.893(95%置信区间 0.843 至 0.943)。对于两年的样本,AUC 在每个级别上区分了被收入开放式病房、低安全单位或中/高安全服务的患者。开放式病房与低安全单位 AUC=0.805(95%CI 0.680 至 0.930);低安全与中/高安全 AUC=0.866,(95%CI 0.784 至 0.949)。所有 11 项指标与结果均呈显著相关。
当根据实际结果对 DUNDRUM-1 分诊安全量表及其各项指标进行测试时,它们达到了标准水平。该工具可用于确保在决定将谁收治到安全的法医医院时决策的一致性。它还可以用于服务和司法管辖区之间的入院门槛进行基准测试。在这项研究中,我们发现评估的需求与实际安置之间存在一些差异。这为未来的研究以及评估未满足的需求、审核病例组合和规划护理途径提供了肥沃的土壤。