Regional Medical Research Centre (ICMR), Bhubaneswar, India.
Indian J Med Res. 2011 Mar;133(3):316-21.
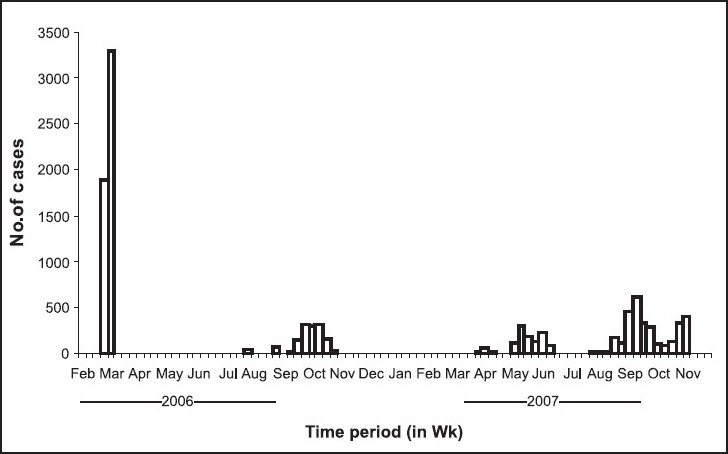
BACKGROUND & OBJECTIVES: A large number of cases of undiagnosed fever and joint pain were reported from different parts of the State of Orissa since February 2006. Epidemiological and laboratory investigation were carried out to confirm the cause of emerging illness, which was provisionally suspected as Chikungunya (CHIK) fever.
Upon getting the reports of suspected CHIK like illness in different parts of the State, epidemic investigations were carried out in the outbreak affected villages. Case history was recorded, clinical examination undertaken and blood samples collected for seroconfirmation for CHIK IgM antibody using ELISA based kit. Simultaneously vector survey was also carried out.
With no previous record of CHIK infection in the State, the first outbreak was confirmed during February 2006. Subsequently, the infection spread to 13 of 30 districts in different episodes covering 79 villages till November 2007. Attack rate was 9-43 per cent in the different outbreaks with average seropositivity of 24 per cent to CHIK specific IgM. Morbidity was high though no deaths were recorded. Aedes aegypti and Ae. albopictus were identified as the possible vectors for transmission.
INTERPRETATION & CONCLUSIONS: The report confirmed emergence of CHIK infection in the State of Orissa, India, and its spread to a larger geographic zone in a short period which warrants public health measures to control further spread.
自 2006 年 2 月以来,印度奥里萨邦不同地区报告了大量不明原因发热和关节痛病例。开展了流行病学和实验室调查以确认新出现疾病的病因,该病被暂时怀疑为基孔肯雅热(CHIK)。
在接到该邦不同地区疑似 CHIK 样疾病报告后,在受疫情影响的村庄开展了疫情调查。记录病例病史,进行临床检查,并采集血液样本,使用 ELISA 试剂盒进行血清学确证,以检测 CHIK IgM 抗体。同时还开展了病媒调查。
由于该邦以前没有 CHIK 感染记录,首次疫情于 2006 年 2 月得到确认。随后,感染在不同时期传播到 30 个区中的 13 个,覆盖了 79 个村庄,直到 2007 年 11 月。不同疫情的发病率为 9-43%,平均 CHIK 特异性 IgM 血清阳性率为 24%。发病率高,但无死亡记录。埃及伊蚊和白纹伊蚊被确定为可能的传播媒介。
该报告确认了 CHIK 感染在印度奥里萨邦的出现,并在短时间内传播到更大的地理区域,这需要采取公共卫生措施来控制进一步传播。