Cardiologie, Centre Hospitalier Universitaire de Caen, Avenue Côte de Nacre, 14033 Caen, Normandy, France.
Crit Care. 2011;15(2):R103. doi: 10.1186/cc10119. Epub 2011 Mar 28.
In pulmonary embolism (PE) without hemodynamic compromise, the prognostic value of right ventricular (RV) dysfunction as measured by echocardiography, computed tomography (CT) or biological (natriuretic peptides) markers has only been assessed in small studies.
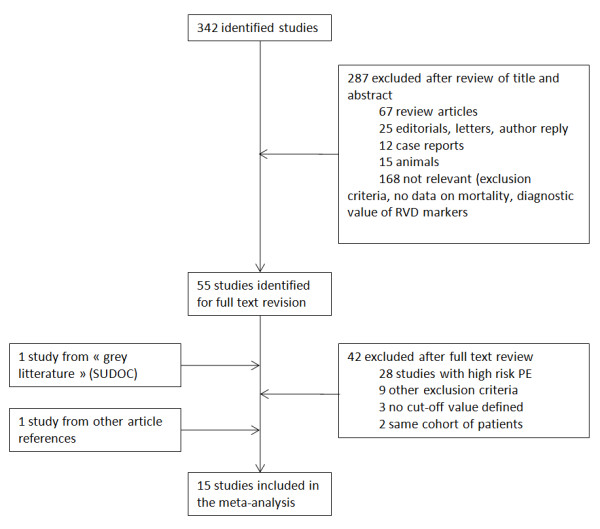
Databases were searched using the combined medical subject headings for right ventricular dysfunction or right ventricular dilatation with the exploded term acute pulmonary embolism. This retrieved 8 echocardiographic marker based studies (n = 1249), three CT marker based studies (n = 503) and 7 natriuretic peptide based studies (n = 582). A meta-analysis of these data was performed with the primary endpoint of mortality within three months after pulmonary embolism, and a secondary endpoint of overall mortality and morbidity by pulmonary embolism.
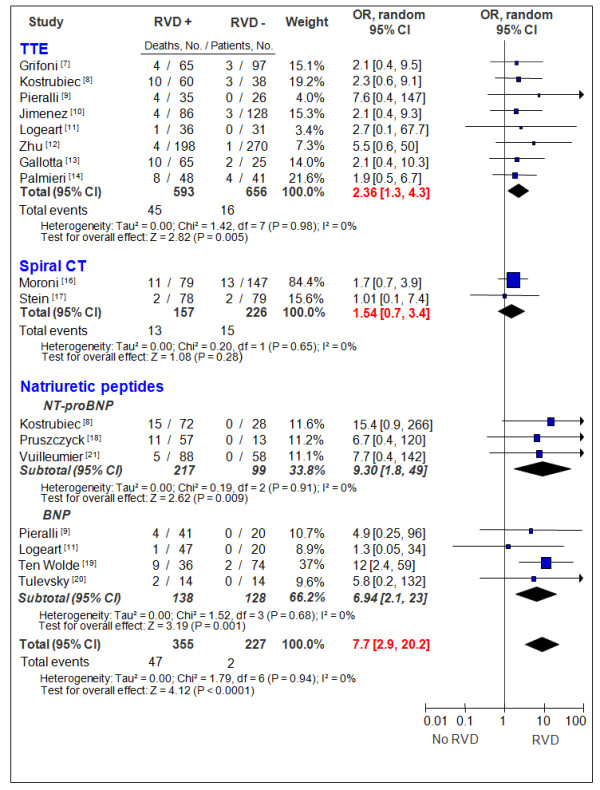
Patients with PE without hemodynamic compromise on admission and the presence of RV dysfunction determined by echocardiography and biological markers were associated with increased short-term mortality (odds ratio (OR) ECHO = 2.36; 95% confidence interval (CI): 1.3-43; OR BNP = 7.7; 95% CI: 2.9-20) while CT was not (ORCT = 1.54-95% CI: 0.7-3.4). However, corresponding pooled negative and positive likelihood ratios independent of death rates were unsatisfactory for clinical usefulness in risk stratification.
The presence of echocardiographic RV dysfunction or elevated natriuretic peptides is associated with short-term mortality in patients with pulmonary embolism without hemodynamic compromise. In contrast, the prognostic value of RV dilation on CT has yet to be validated in this population. As indicated both by positive and negative likelihood ratios the current prognostic value in clinical practice remains very limited.
在无血流动力学障碍的肺栓塞(PE)中,超声心动图、计算机断层扫描(CT)或生物标志物(利钠肽)测定的右心室(RV)功能障碍的预后价值仅在一些小型研究中进行了评估。
使用联合医学主题词,通过超声心动图标记右心室功能障碍或右心室扩张,用展开项急性肺栓塞检索数据库。这共检索到 8 项基于超声心动图标志物的研究(n = 1249)、3 项基于 CT 标志物的研究(n = 503)和 7 项基于利钠肽的研究(n = 582)。对这些数据进行了荟萃分析,主要终点为 PE 后三个月内的死亡率,次要终点为 PE 的总死亡率和发病率。
入院时无血流动力学障碍且存在 RV 功能障碍的 PE 患者,通过超声心动图和生物标志物确定,与短期死亡率增加相关(ECHO 的比值比(OR)= 2.36;95%置信区间(CI):1.3-43;BNP 的 OR = 7.7;95% CI:2.9-20),而 CT 则不然(ORCT = 1.54-95% CI:0.7-3.4)。然而,独立于死亡率的汇总阴性和阳性似然比在风险分层中的临床应用并不理想。
在无血流动力学障碍的 PE 患者中,超声心动图 RV 功能障碍或利钠肽升高与短期死亡率相关。相比之下,CT 上 RV 扩张的预后价值尚未在该人群中得到验证。正如阳性和阴性似然比所表明的,目前在临床实践中的预后价值仍然非常有限。