Amucheazi A O, Ajuzeiogu V O, Ezike H A, Odiakosa M C, Nwoke O M, Onyia E
Department of Anaesthesia, University of Nigeria Teaching Hospital, Ituku-Ozalla, Nigeria.
Asian J Transfus Sci. 2011 Jan;5(1):35-8. doi: 10.4103/0973-6247.75984.
GENERAL OBJECTIVE: To assess the practice of blood conservation.
To determine the methods of blood conservation in use, to assess the lower limit for hemoglobin for elective procedures, to determine transfusion trigger point in practice, to find out limitations in practice and ways to improve clinical practice.
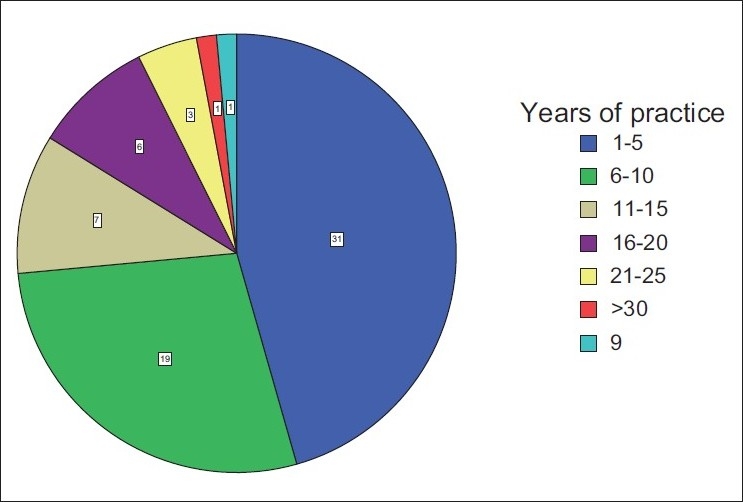
This was conducted in February 2009. Self-administered questionnaires were distributed among the surgeons and anesthetists in practice at the University of Nigeria Teaching Hospital, Enugu State University Teaching Hospital, Ebonyi State University Teaching Hospital and National Orthopaedic Hospital, Enugu. The data gathered was analyzed using the SPSS software.
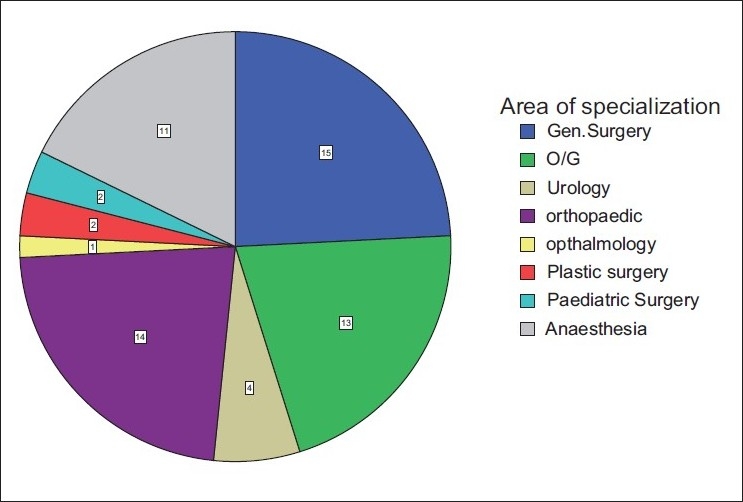
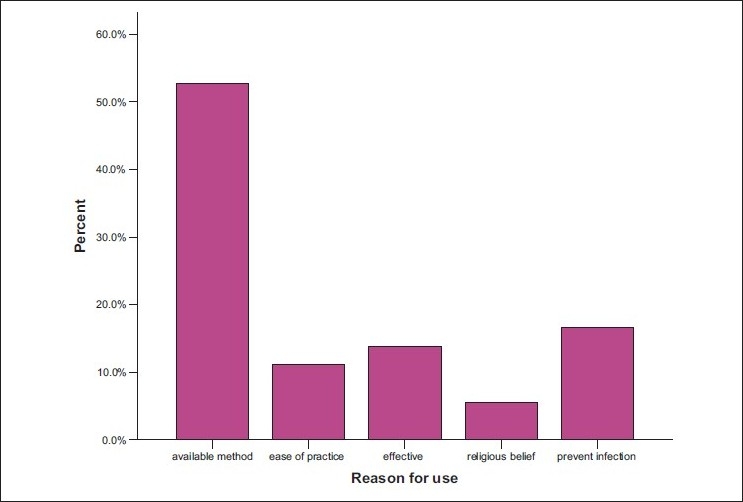
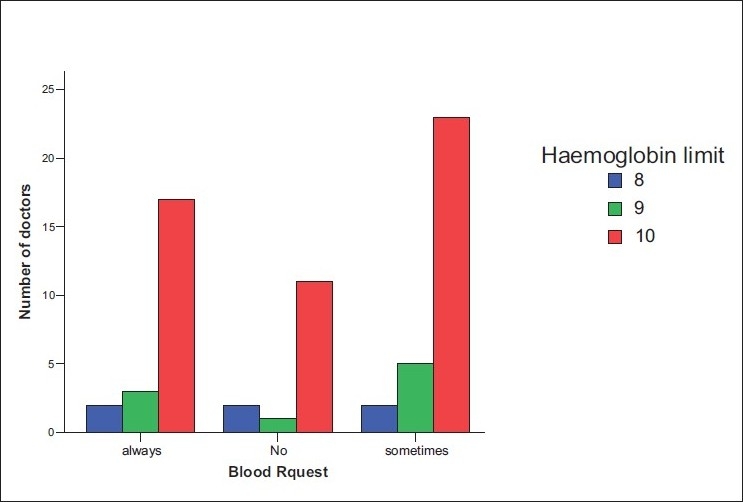
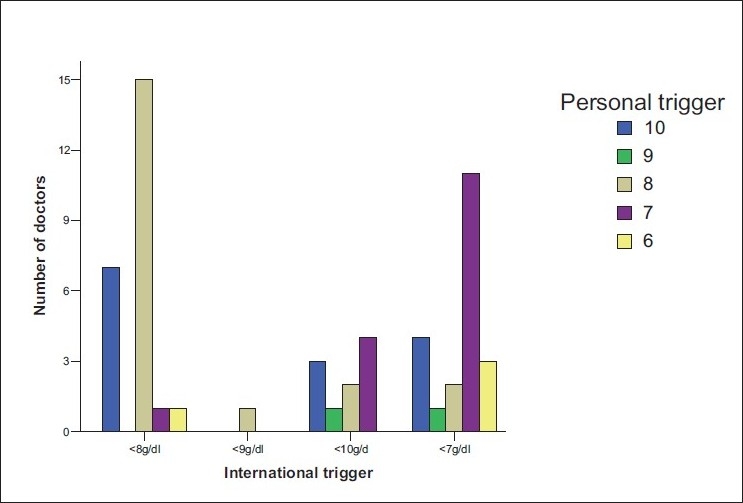
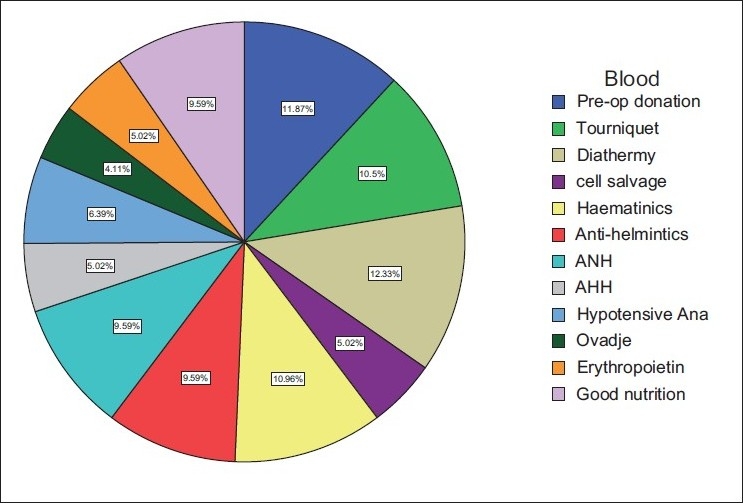
: Of participants who agreed to fill the questionnaires, more than 50% were males. The most prevalent specialty was general surgery (24.2%), followed by orthopedics (22.6%), obstetrics and gynecology (20.7%), and anesthesia (17.7%). The lowest hemoglobin limit before the patient was allowed into the theatre for elective procedures was 10 g/dl while individual transfusion trigger points ranged from hemoglobin of 6 to 10 g/dl. Majority of the doctors would avoid homologous blood transfusion in order to avoid transfusion-related diseases and reaction. Regarding knowledge of blood conservation methods and means of avoiding homologous blood, the use of diathermy was highest (12.33%), followed by preoperative blood donation (11.87%), use of hematinics (10.96%), and tourniquet 10.5%. Also, in practice, diathermy was the most frequently used (18.69%), followed by preoperative blood donation (16.16%), use of tourniquet (15.15%), while the Ovadje cell saver was least with 0.01%. Suggestions from respondents on the ways of limiting transfusion-related problems included optimization of patients (24.5%), improvement of standard of living (17.7%), and personnel training (13.3%).
There is an agreement with the global trend geared toward minimizing the use of homologous blood by doctors in these hospitals. However, our practice must continually be refined by continuing medical education in order to keep everyone informed of changes in practice. The Government must improve the quality of service by the provision of unavailable infrastructure.
评估血液保护措施的实施情况。
确定所使用的血液保护方法,评估择期手术血红蛋白下限,确定实际输血触发点,找出实际操作中的限制因素以及改善临床实践的方法。
该研究于2009年2月开展。自行填写的问卷被分发给尼日利亚大学教学医院、埃努古州立大学教学医院、埃邦伊州立大学教学医院和埃努古国家骨科医院的外科医生和麻醉师。收集到的数据使用SPSS软件进行分析。
同意填写问卷的参与者中,超过50%为男性。最常见的专业是普通外科(24.2%),其次是骨科(22.6%)、妇产科(20.7%)和麻醉科(17.7%)。择期手术患者进入手术室前的最低血红蛋白下限为10g/dl,而个体输血触发点的血红蛋白范围为6至10g/dl。大多数医生会避免输注同源血以避免输血相关疾病和反应。关于血液保护方法和避免同源血使用的知识,使用电刀的比例最高(12.33%),其次是术前自体献血(11.87%)、使用补血剂(10.96%)和止血带(10.5%)。此外,在实际操作中,电刀使用最为频繁(18.69%),其次是术前自体献血(16.16%)、使用止血带(15.15%),而奥瓦德血液回收机最少,仅为0.01%。受访者关于限制输血相关问题的建议包括优化患者状况(24.5%)、改善生活水平(17.7%)和人员培训(13.3%)。
这些医院的医生在减少同源血使用方面与全球趋势一致。然而,我们的实践必须通过继续医学教育不断完善,以便让每个人了解实践中的变化。政府必须通过提供缺失的基础设施来提高服务质量。