Department of Health Policy, Management and Evaluation, Faculty of Medicine, University of Toronto, Guelph, ON, Canada.
BMC Med. 2011 May 18;9:58. doi: 10.1186/1741-7015-9-58.
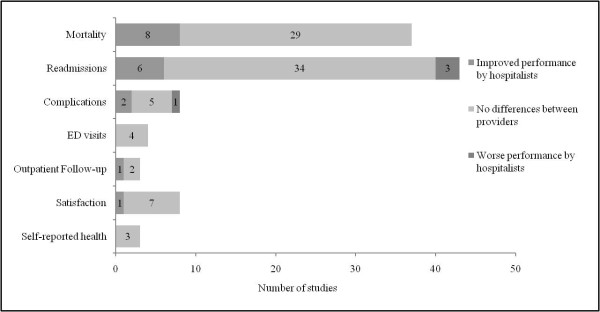
Despite more than a decade of research on hospitalists and their performance, disagreement still exists regarding whether and how hospital-based physicians improve the quality of inpatient care delivery. This systematic review summarizes the findings from 65 comparative evaluations to determine whether hospitalists provide a higher quality of inpatient care relative to traditional inpatient physicians who maintain hospital privileges with concurrent outpatient practices.
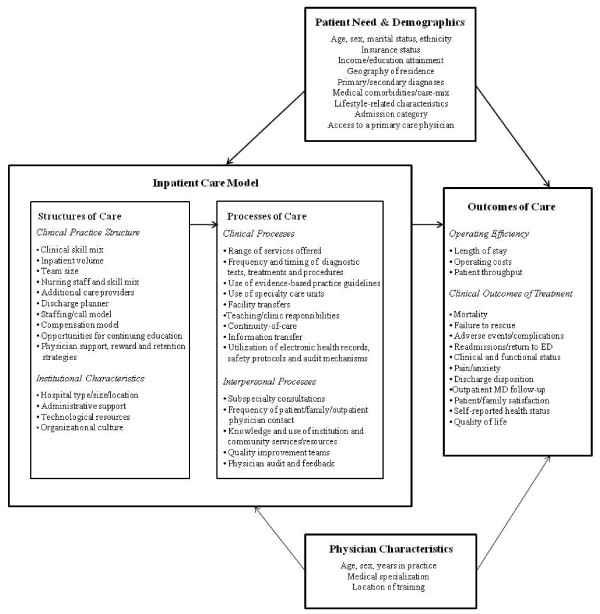
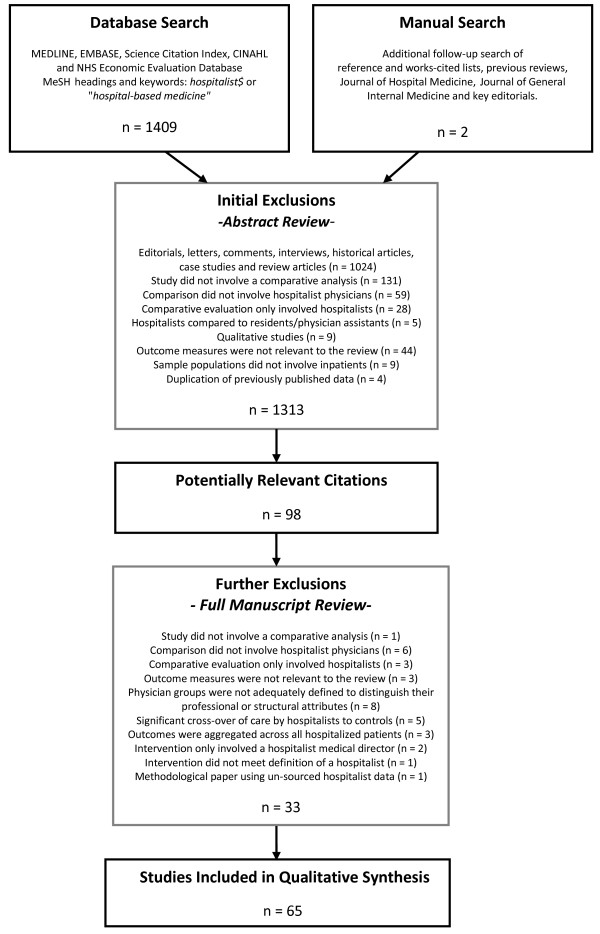
Articles on hospitalist performance published between January 1996 and December 2010 were identified through MEDLINE, Embase, Science Citation Index, CINAHL, NHS Economic Evaluation Database and a hand-search of reference lists, key journals and editorials. Comparative evaluations presenting original, quantitative data on processes, efficiency or clinical outcome measures of care between hospitalists, community-based physicians and traditional academic attending physicians were included (n = 65). After proposing a conceptual framework for evaluating inpatient physician performance, major findings on quality are summarized according to their percentage change, direction and statistical significance.
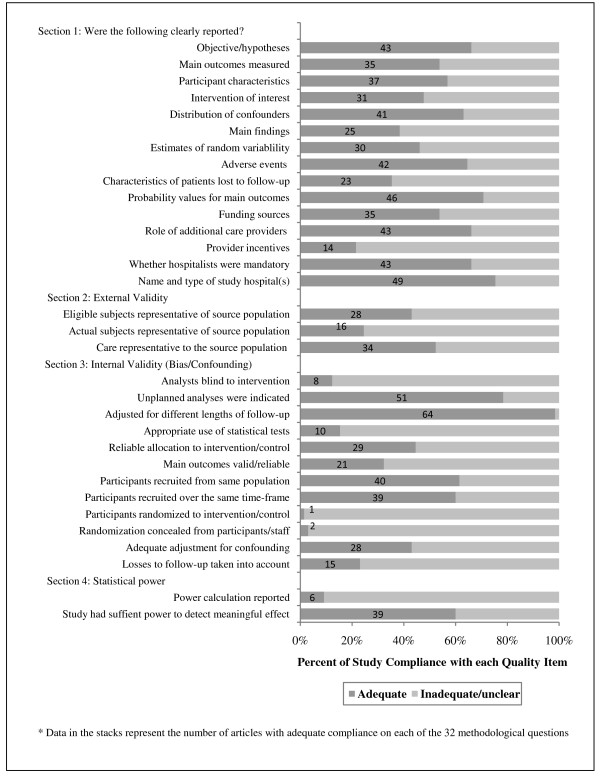
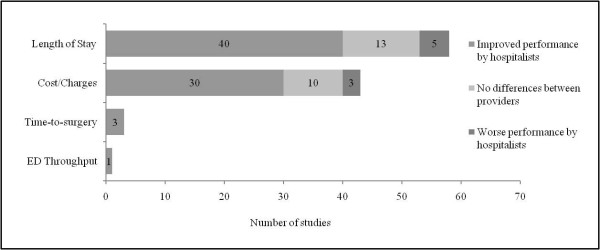
The majority of reviewed articles demonstrated that hospitalists are efficient providers of inpatient care on the basis of reductions in their patients' average length of stay (69%) and total hospital costs (70%); however, the clinical quality of hospitalist care appears to be comparable to that provided by their colleagues. The methodological quality of hospitalist evaluations remains a concern and has not improved over time. Persistent issues include insufficient reporting of source or sample populations (n = 30), patients lost to follow-up (n = 42) and estimates of effect or random variability (n = 35); inappropriate use of statistical tests (n = 55); and failure to adjust for established confounders (n = 37).
Future research should include an expanded focus on the specific structures of care that differentiate hospitalists from other inpatient physician groups as well as the development of better conceptual and statistical models that identify and measure underlying mechanisms driving provider-outcome associations in quality.
尽管对医院医师及其绩效进行了十余年的研究,但仍存在争议,即基于医院的医生是否以及如何提高住院患者护理的质量。本系统评价总结了 65 项比较评估的结果,以确定医院医师相对于同时保留门诊实践的传统住院医师是否以及如何提供更高质量的住院患者护理。
通过 MEDLINE、Embase、科学引文索引、CINAHL、NHS 经济评价数据库以及对参考文献、主要期刊和社论的手工搜索,确定了 1996 年 1 月至 2010 年 12 月期间发表的有关医院医师绩效的文章。纳入了比较评价的文章,这些文章提供了有关医院医师、社区医师和传统学术主治医生之间的护理过程、效率或临床结果措施的原始、定量数据(n = 65)。在提出评估住院医师绩效的概念框架后,根据质量的百分比变化、方向和统计学意义总结了主要发现。
大多数综述文章表明,医院医师是高效的住院患者护理提供者,这是基于患者平均住院时间(69%)和总住院费用(70%)的减少;然而,医院医师护理的临床质量似乎与同事提供的护理质量相当。医院医师评价的方法学质量仍然是一个问题,而且随着时间的推移并没有得到改善。持续存在的问题包括来源或样本人群的报告不足(n = 30)、患者失访(n = 42)以及效果或随机变异性的估计(n = 35);统计检验的不当使用(n = 55);以及未能调整既定混杂因素(n = 37)。
未来的研究应扩大重点,关注区分医院医师和其他住院医师群体的具体护理结构,以及开发更好的概念和统计模型,以确定和衡量推动质量中提供者-结果关联的潜在机制。