Department for Infectious Disease Epidemiology, Robert Koch Institute, Berlin, Germany.
BMC Public Health. 2011 Jun 15;11:474. doi: 10.1186/1471-2458-11-474.
In Germany, measles vaccination coverage with two doses is not yet sufficient to prevent regional outbreaks. Among the 16 German federal states, vaccination coverage was lowest in Bavaria with 85% in 2008. From March to mid-April 2008, four neighbouring Bavarian counties reported 55 measles-cases mostly linked to an ongoing measles outbreak in an anthroposophic school in Austria. We investigated this outbreak to guide future public health action.
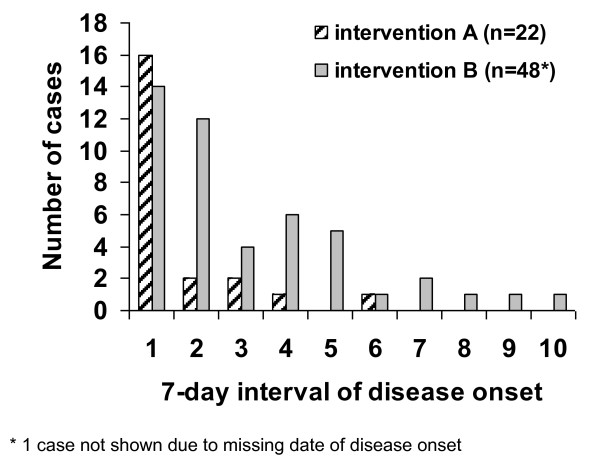
We applied the German national case-definition for measles and collected data using the national surveillance system and a questionnaire. Measles cases with disease onset a maximum of 18 days apart and spatial contact (e.g. same household, same school) were summed up in clusters. Two different interventions, which were implemented in schools and kindergartens in Bavaria, were compared by their impact on the size and duration of measles clusters. Susceptible persons were excluded from schools or kindergartens either with the first (intervention A) or second (intervention B) measles case occurring in the respective institution.
Among the 217 Bavarian measles cases identified from March-July 2008, 28 (13%) cases were attendees of the anthroposophic school in Austria. In total, vaccination status was known in 161 (74%) cases and 156 (97%) of them were not vaccinated. The main factor for non-vaccination was "fear of vaccine-related adverse events" (33%). Twenty-nine (18%) of 161 cases suffered complications. Exclusively genotype D5 was detected. Overall, 184 cases could be epidemiologically grouped into 59 clusters. Of those, 41 clusters could be linked to households and 13 to schools or kindergartens. The effect of intervention A and B was analysed in 10 school or kindergarten clusters. Depending on the respective intervention A or B, the median number of cases per cluster was 3 versus 13 (p = 0.05), and the median duration of a cluster was 3 versus 26 days (p = 0.13).
Introduction of measles virus into a pocket of susceptible persons (e.g. vaccination opponents or sceptics) may lead to large outbreaks in the general population, if the general population's vaccination coverage is below the WHO recommended level. Education on the safety of measles vaccine needs to be strengthened to increase measles vaccination coverage. Early intervention may limit spread in schools or kindergartens. Suspected measles has to be reported immediately to the local health authorities in order to allow intervention as early as possible.
在德国,两剂麻疹疫苗的接种覆盖率还不足以防止区域性爆发。在 16 个联邦州中,巴伐利亚州的疫苗接种覆盖率最低,2008 年为 85%。2008 年 3 月至 4 月中旬,巴伐利亚的四个相邻县报告了 55 例麻疹病例,主要与奥地利一所人智学学校正在发生的麻疹爆发有关。我们调查了此次疫情,以指导未来的公共卫生行动。
我们应用了德国国家麻疹病例定义,并通过国家监测系统和问卷调查收集数据。将发病时间相隔最多 18 天且具有空间接触(例如,同住一个家庭,同校就读)的麻疹病例汇总为聚集病例。在巴伐利亚的学校和幼儿园中实施了两种不同的干预措施,通过比较它们对麻疹聚集病例的大小和持续时间的影响来评估其效果。通过在各自机构中出现第一例(干预 A)或第二例(干预 B)麻疹病例,将易感者排除在学校或幼儿园之外。
在 2008 年 3 月至 7 月期间从巴伐利亚州确定的 217 例麻疹病例中,28 例(13%)为奥地利人智学学校的学生。总共已知 161 例(74%)的接种情况,其中 156 例(97%)未接种。不接种疫苗的主要原因是“对疫苗相关不良反应的恐惧”(33%)。29 例(18%)病例出现并发症。仅检测到基因型 D5。总体而言,184 例病例可以在流行病学上分为 59 个聚集病例。其中,41 个聚集病例与家庭有关,13 个与学校或幼儿园有关。分析了干预 A 和 B 对 10 个学校或幼儿园聚集病例的影响。根据各自的干预 A 或 B,每个聚集病例的中位数分别为 3 例和 13 例(p = 0.05),每个聚集病例的持续时间中位数分别为 3 天和 26 天(p = 0.13)。
如果人群的疫苗接种覆盖率低于世界卫生组织建议的水平,将麻疹病毒引入易感人群(例如,疫苗反对者或怀疑论者)可能会导致人群中爆发大规模疫情。需要加强麻疹疫苗安全性方面的教育,以提高麻疹疫苗的接种率。早期干预可能会限制学校或幼儿园中的传播。一旦出现疑似麻疹病例,必须立即向当地卫生当局报告,以便尽早进行干预。