Department of Obstetrics and Gynaecology, Aarhus University Hospital, Skejby, Aarhus, Denmark.
BMC Womens Health. 2011 Jun 23;11:31. doi: 10.1186/1472-6874-11-31.
Ovarian cancer is the leading cause of death among women suffering from gynaecological malignancies in the Western world. Worldwide, approximately 200,000 women are diagnosed with the disease each year. This article deals with the health care seeking and symptom interpretation process among Danish women, who have a very high mortality rate.
The health seeking and symptom interpretation process was analysed via combining study methods. The material consisted of registry data dealing with the use of public health care and hospital services of Danish women, newly diagnosed with ovarian cancer. These results were combined with findings from semi-structured qualitative research interviews on women's bodily experiences with symptom development.
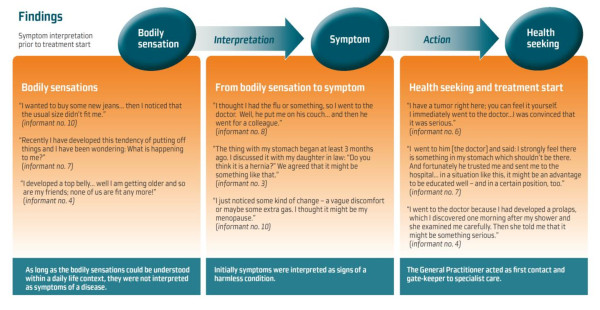
A number of 663 Danish women with ovarian cancer attended 27 different kinds of primary health care providers in a total of 14,009 visits during 2007. The women also had 6,214 contacts with various hospitals, and obtained 562 different diagnoses.From the main theme "Women's experiences with the onset of symptoms" three sub-themes were identified: "Bodily sensations", "From bodily sensation to symptom", and "Health seeking and treatment start". In all cases the General Practitioner represented the first contact to public health care, acting as gate-keeper to specialist and hospital referral.The women were major users of public health care throughout the diagnostic process and subsequent treatment. All women held personal knowledge concerning the onset of their symptoms. The early symptoms of ovarian cancer might be uncharacteristic and non-disease-specific when interpreted as personal experiences, but they had similarities when analysed together.
Diagnostic delay in ovarian cancer seems far from being exclusively a medical problem, as the delay proved to be influenced by organisational, cultural, and social factors, too. Initiatives facilitating the diagnostic process and research concerning the selection of individuals for further investigation are indicated. The way in which the women interpreted their symptoms was influenced by their personal experiences, their cultural, and their social background. This became crucial to the diagnostic process. These issues need to be explored through further research on women's experiences during the diagnostic process.
在西方世界,卵巢癌是妇科恶性肿瘤导致女性死亡的主要原因。全球范围内,每年约有 20 万名女性被诊断患有该病。本文研究的是丹麦女性的医疗保健寻求和症状解释过程,这些女性的死亡率非常高。
通过结合研究方法分析了医疗保健寻求和症状解释过程。该材料包括丹麦新诊断为卵巢癌的女性在 2007 年期间使用公共医疗保健和医院服务的登记数据。这些结果与关于女性身体症状发展的半结构化定性研究访谈的结果相结合。
共有 663 名丹麦卵巢癌女性在 27 种不同的初级保健提供者处就诊,总就诊次数为 14009 次。这些女性还与各种医院有 6214 次接触,并获得了 562 种不同的诊断。从“女性对症状发作的体验”这一主要主题中,确定了三个子主题:“身体感觉”、“从身体感觉到症状”和“医疗保健寻求和治疗开始”。在所有情况下,全科医生都是公共医疗保健的第一接触者,充当专家和医院转诊的把关人。女性在整个诊断过程和随后的治疗中都是公共医疗保健的主要使用者。所有女性都对自己症状的发作有个人了解。卵巢癌的早期症状可能是非典型的,也不是特定于疾病的,如果将其解释为个人经历,那么这些症状可能没有特异性,但当一起分析时,它们具有相似性。
卵巢癌的诊断延迟似乎远非仅仅是一个医学问题,因为延迟也受到组织、文化和社会因素的影响。需要采取措施促进诊断过程,并开展关于选择进一步调查对象的研究。女性对自己症状的解释方式受到个人经历、文化和社会背景的影响。这对诊断过程至关重要。这些问题需要通过进一步研究女性在诊断过程中的经历来探讨。