Allergy and Immunology Section, Division of Pulmonary, Allergy, and Critical Care Medicine, University of Pennsylvania, Philadelphia, PA, USA.
J Allergy Clin Immunol. 2011 Sep;128(3):516-23.e1-5. doi: 10.1016/j.jaci.2011.05.010. Epub 2011 Jun 25.
Improving inhaled corticosteroid (ICS) adherence should improve asthma outcomes.
In a randomized controlled trial we tested whether an individualized problem-solving (PS) intervention improves ICS adherence and asthma outcomes.
Adults with moderate or severe asthma from clinics serving urban neighborhoods were randomized to PS (ie, defining specific barriers to adherence, proposing/weighing solutions, trying the best, assessing, and revising) or standard asthma education (AE) for 3 months and then observed for 3 months. Adherence was monitored electronically. Outcomes included the following: asthma control, FEV(1), asthma-related quality of life, emergency department (ED) visits, and hospitalizations. In an intention-to-treat-analysis longitudinal models using random effects and regression were used.
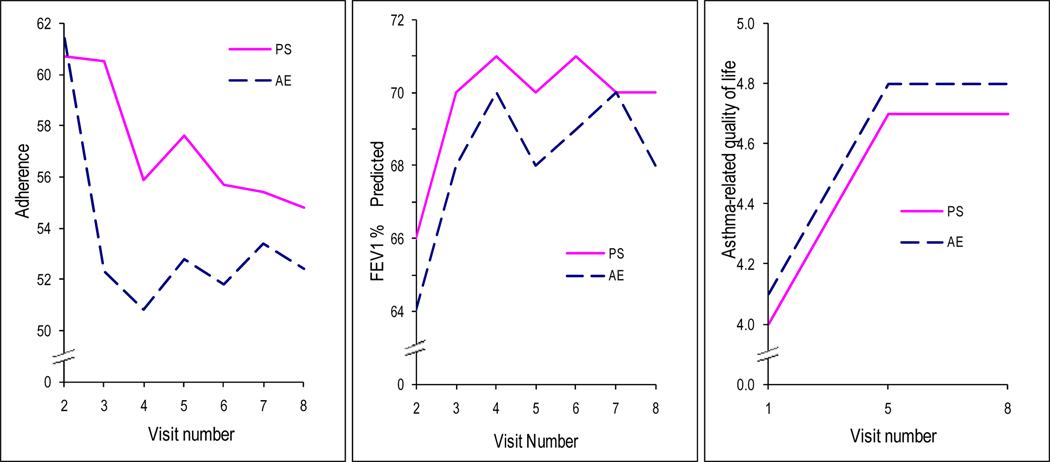
Three hundred thirty-three adults were randomized: 49 ± 14 years of age, 72% female, 68% African American, 7% Latino, mean FEV(1) of 66% ± 19%, and 103 (31%) with hospitalizations and 172 (52%) with ED visits for asthma in the prior year. There was no difference between groups in overall change in any outcome (P > .20). Mean adherence (61% ± 27%) decreased significantly (P = .0004) over time by 14% and 10% in the AE and PS groups, respectively. Asthma control improved overall by 15% (P = .002). In both groups FEV(1) and quality of life improved by 6% (P = .01) and 18% (P < .0001), respectively. However, the improvement in FEV(1) only occurred during monitoring but not subsequently after randomization. Rates of ED visits and hospitalizations did not significantly decrease over the study period.
PS was not better than AE in improving adherence or asthma outcomes. However, monitoring ICS use with provision of medications and attention, which was imposed on both groups, was associated with improvement in FEV(1) and asthma control.
提高吸入性皮质类固醇(ICS)的依从性应该可以改善哮喘的结果。
我们在一项随机对照试验中测试了个体化问题解决(PS)干预是否可以提高 ICS 的依从性和哮喘结果。
从服务于城市社区的诊所招募患有中度或重度哮喘的成年人,将他们随机分为 PS(即确定特定的依从性障碍,提出/权衡解决方案,尝试最佳方案,评估和修订)或标准哮喘教育(AE)组,干预时长为 3 个月,然后进行 3 个月的观察。通过电子方式监测依从性。结果包括以下方面:哮喘控制、FEV1、哮喘相关生活质量、急诊室(ED)就诊次数和住院次数。在意向治疗分析中,使用随机效应和回归的纵向模型进行分析。
共 333 名成年人被随机分配:年龄 49 ± 14 岁,女性占 72%,非裔美国人占 68%,拉丁裔占 7%,平均 FEV1 为 66% ± 19%,过去一年中,103 人(31%)因哮喘住院,172 人(52%)因哮喘到 ED 就诊。两组在任何结局的总体变化上均无差异(P >.20)。AE 组和 PS 组的依从性分别平均下降了 14%和 10%(P =.0004),这表明依从性随时间显著下降。哮喘控制总体上改善了 15%(P =.002)。在两组中,FEV1 和生活质量分别改善了 6%(P =.01)和 18%(P <.0001)。然而,FEV1 的改善仅发生在监测期间,而在随机分组后并未持续。在整个研究期间,ED 就诊和住院的次数并没有显著减少。
PS 并不优于 AE 改善依从性或哮喘结果。然而,对两组都实施的监测 ICS 使用情况、提供药物和关注与 FEV1 和哮喘控制的改善有关。