Université François Rabelais de Tours, Centre National de la Recherche Scientifique UMR 6239 GICC, 3 rue des Tanneurs, F-37041 Tours Cedex 1, France.
Arthritis Res Ther. 2011 Jun 27;13(3):R105. doi: 10.1186/ar3386.
A proportion of patients receiving infliximab have antibodies toward infliximab (ATI), which are associated with increased risk of infusion reaction and reduced response to treatment. We studied the association of infliximab concentration at treatment initiation and development of ATI as well as the association of the presence of ATI and maintenance of infliximab.
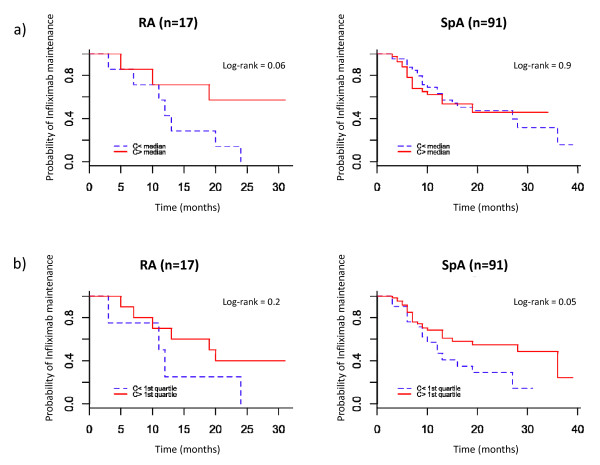
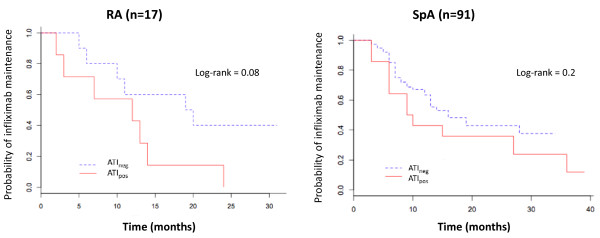
All patients with rheumatoid arthritis (RA) or spondyloarthritis (SpA) receiving infliximab beginning in December 2005 were retrospectively followed until January 2009 or until infliximab discontinuation. Trough serum infliximab and ATI concentrations were measured at each visit. The patients were separated into two groups: ATI(pos) if ATI were detected at least once during the follow-up period and ATI(neg) otherwise. Repeated measures analysis of variance was used to study the association of infliximab concentration at treatment initiation and the development of ATI. Maintenance of infliximab in the two groups was studied by using Kaplan-Meier curves.
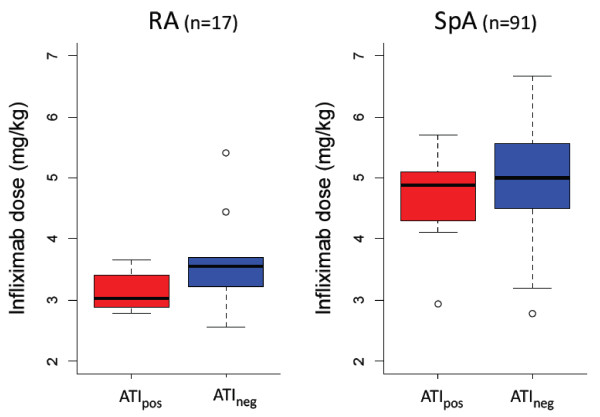
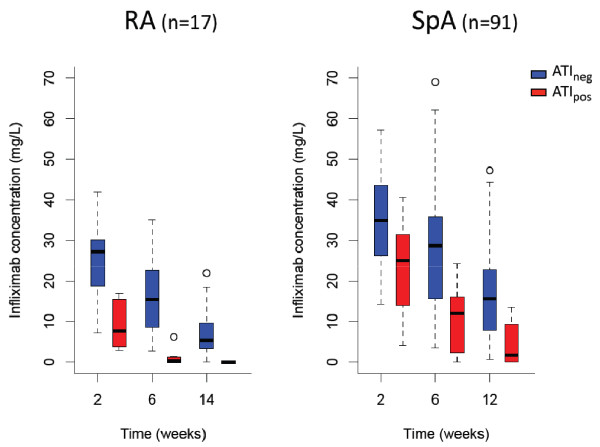
We included 108 patients: 17 with RA and 91 with SpA. ATI were detected in 21 patients (19%). The median time to ATI detection after initiation of infliximab was 3.7 months (1.7 to 26.0 months). For both RA and SpA patients, trough infliximab concentration during the initiation period was significantly lower for ATI(pos) than ATI(neg) patients. RA patients showed maintenance of infliximab at a median of 19.5 months (5.0 to 31.0 months) and 12.0 months (2.0 to 24.0 months) for ATI(neg) and ATI(pos) groups, respectively (P = 0.08). SpA patients showed infliximab maintenance at a median of 16.0 months (3.0 to 34.0 months) and 9.5 months (3.0 to 39.0 months) for ATI(neg) and ATI(pos) groups, respectively (P = 0.20). Among SpA patients, those who were being treated concomitantly with methotrexate had a lower risk of developing ATI than patients not taking methotrexate (0 of 14 patients (0%) vs. 25 of 77 patients (32%); P = 0.03).
High concentrations of infliximab during treatment initiation reduce the development of ATI, and the absence of ATI may be associated with prolonged maintenance of infliximab. Thus, trough serum infliximab concentration should be monitored early in patients with rheumatic diseases.
一部分接受英夫利昔单抗治疗的患者会产生针对英夫利昔单抗的抗体(ATI),这与输注反应风险增加和治疗应答降低有关。我们研究了治疗起始时英夫利昔单抗浓度与 ATI 发展之间的关系,以及 ATI 存在与英夫利昔单抗维持之间的关系。
所有于 2005 年 12 月开始接受英夫利昔单抗治疗的类风湿关节炎(RA)或脊柱关节炎(SpA)患者均进行回顾性随访,直至 2009 年 1 月或直至英夫利昔单抗停药。在每次就诊时测量血清英夫利昔单抗和 ATI 浓度。患者分为两组:ATI(pos)如果在随访期间至少检测到一次 ATI,否则为 ATI(neg)。采用重复测量方差分析研究治疗起始时英夫利昔单抗浓度与 ATI 发展之间的关系。采用 Kaplan-Meier 曲线研究两组中英夫利昔单抗的维持情况。
我们纳入了 108 例患者:17 例 RA 患者和 91 例 SpA 患者。21 例(19%)患者检测到 ATI。英夫利昔单抗起始后检测到 ATI 的中位时间为 3.7 个月(1.7 至 26.0 个月)。对于 RA 和 SpA 患者,ATI(pos)患者的起始期血清英夫利昔单抗浓度明显低于 ATI(neg)患者。RA 患者的英夫利昔单抗维持中位数为 19.5 个月(5.0 至 31.0 个月)和 12.0 个月(2.0 至 24.0 个月),分别为 ATI(neg)和 ATI(pos)组(P = 0.08)。SpA 患者的英夫利昔单抗维持中位数分别为 16.0 个月(3.0 至 34.0 个月)和 9.5 个月(3.0 至 39.0 个月),分别为 ATI(neg)和 ATI(pos)组(P = 0.20)。在 SpA 患者中,同时接受甲氨蝶呤治疗的患者发生 ATI 的风险低于未接受甲氨蝶呤治疗的患者(0/14 例(0%)比 25/77 例(32%);P = 0.03)。
治疗起始时高浓度的英夫利昔单抗可降低 ATI 的发展,而不存在 ATI 可能与英夫利昔单抗的维持时间延长有关。因此,应早期监测风湿性疾病患者的血清英夫利昔单抗浓度。