Laboratorio de Enfermedades Autoinmunes Josep Font, IDIBAPS, Hospital Clínic, C/Villarroel, Barcelona, 08036, Spain.
Arthritis Res Ther. 2011 Jul 11;13(4):R112. doi: 10.1186/ar3397.
The purpose of this observational study was to analyze the rates, characteristics and associated risk factors of severe infections in patients with systemic autoimmune diseases (SAD) who were treated off-label with biological agents in daily practice.
The BIOGEAS registry is an ongoing Spanish prospective cohort study investigating the long-term safety and efficacy of the off-label use of biological agents in adult patients with severe, refractory SAD. Severe infections were defined according to previous studies as those that required intravenous treatment or that led to hospitalization or death. Patients contributed person-years of follow-up for the period in which they were treated with biological agents.
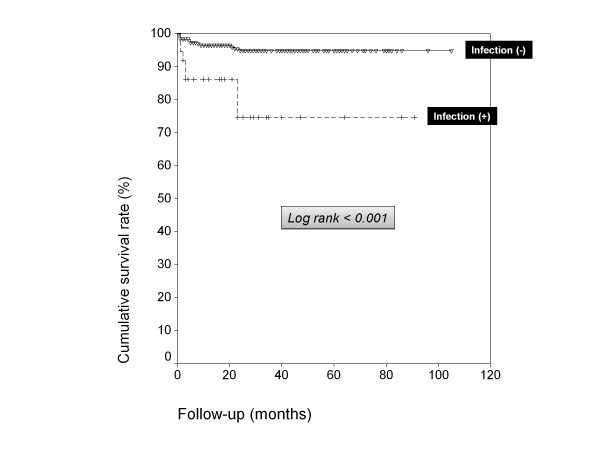
A total of 344 patients with SAD treated with biological agents off-label were included in the Registry until July 2010. The first biological therapies included rituximab in 264 (77%) patients, infliximab in 37 (11%), etanercept in 21 (6%), adalimumab in 19 (5%), and 'other' agents in 3 (1%). Forty-five severe infections occurred in 37 patients after a mean follow-up of 26.76 months. These infections resulted in four deaths. The crude rate of severe infections was 90.9 events/1000 person-years (112.5 for rituximab, 76.9 for infliximab, 66.9 for adalimumab and 30.5 for etanercept respectively). In patients treated with more than two courses of rituximab, the crude rate of severe infection was 226.4 events/1000 person-years. A pathogen was identified in 24 (53%) severe infections. The most common sites of severe infection were the lower respiratory tract (39%), bacteremia/sepsis (20%) and the urinary tract (16%). There were no significant differences relating to gender, SAD, agent, other previous therapies, number of previous immunosuppressive agents received or other therapies administered concomitantly. Cox regression analysis showed that age (P = 0.015) was independently associated with an increased risk of severe infection. Survival curves showed a lower survival rate in patients with severe infections (log-rank and Breslow tests < 0.001).
The rates of severe infections in SAD patients with severe, refractory disease treated depended on the biological agent used, with the highest rates being observed for rituximab and the lowest for etanercept. The rate of infection was especially high in patients receiving three or more courses of rituximab. In patients with severe infections, survival was significantly reduced. Older age was the only significant predictive factor of severe infection.
本观察性研究的目的是分析在日常实践中接受生物制剂的标签外治疗的系统性自身免疫性疾病(SAD)患者中严重感染的发生率、特征和相关危险因素。
BIOGEAS 登记处是一项正在进行的西班牙前瞻性队列研究,旨在调查生物制剂标签外用于治疗严重、难治性 SAD 成年患者的长期安全性和疗效。严重感染根据先前的研究定义为需要静脉治疗或导致住院或死亡的感染。患者在接受生物制剂治疗期间计入随访人年。
截至 2010 年 7 月,该登记处共纳入 344 例接受生物制剂标签外治疗的 SAD 患者。第一批生物治疗药物包括利妥昔单抗 264 例(77%)、英夫利昔单抗 37 例(11%)、依那西普 21 例(6%)、阿达木单抗 19 例(5%)和其他药物 3 例(1%)。在平均随访 26.76 个月后,37 名患者出现 45 例严重感染。这些感染导致 4 例死亡。严重感染的粗发生率为 90.9 例/1000 人年(利妥昔单抗为 112.5 例,英夫利昔单抗为 76.9 例,阿达木单抗为 66.9 例,依那西普为 30.5 例)。在接受两剂以上利妥昔单抗治疗的患者中,严重感染的粗发生率为 226.4 例/1000 人年。在 24 例(53%)严重感染中确定了病原体。严重感染最常见的部位是下呼吸道(39%)、菌血症/败血症(20%)和尿路感染(16%)。性别、SAD、药物、其他先前的治疗、先前接受的免疫抑制剂数量或同时给予的其他治疗无显著差异。Cox 回归分析显示,年龄(P=0.015)与严重感染风险增加独立相关。生存曲线显示严重感染患者的生存率较低(对数秩和 Breslow 检验<0.001)。
在接受生物制剂标签外治疗的严重、难治性 SAD 患者中,严重感染的发生率取决于所用的生物制剂,其中利妥昔单抗的发生率最高,依那西普的发生率最低。接受三剂或更多剂利妥昔单抗治疗的患者感染率尤其高。在严重感染患者中,生存率显著降低。年龄较大是严重感染的唯一显著预测因素。