Douglas Mental Health University Institute, 6875 Bld, Lasalle, Verdun, Montréal (Québec), H4H 1R3, Canada.
BMC Health Serv Res. 2011 Jul 11;11:166. doi: 10.1186/1472-6963-11-166.
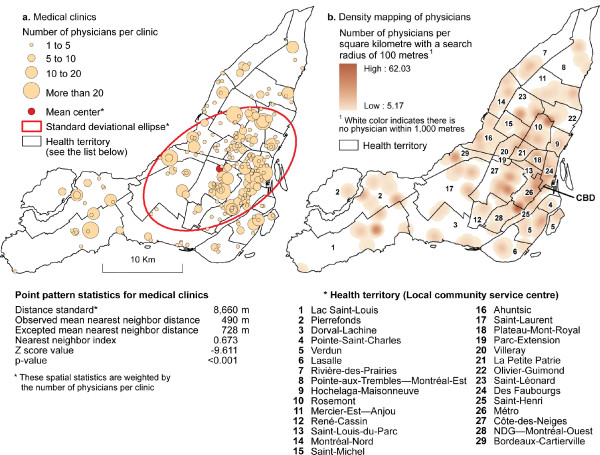
Reducing spatial access disparities to healthcare services is a growing priority for healthcare planners especially among developed countries with aging populations. There is thus a pressing need to determine which populations do not enjoy access to healthcare, yet efforts to quantify such disparities in spatial accessibility have been hampered by a lack of satisfactory measurements and methods. This study compares an optimised and the conventional version of the two-step floating catchment area (2SFCA) method to assess spatial accessibility to medical clinics in Montreal.
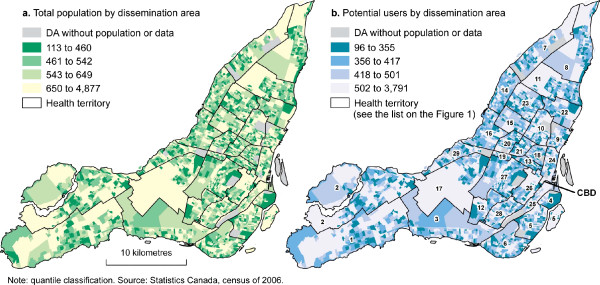
We first computed catchments around existing medical clinics of Montreal Island based on the shortest network distance. Population nested in dissemination areas were used to determine potential users of a given medical clinic. To optimize the method, medical clinics (supply) were weighted by the number of physicians working in each clinic, while the previous year's medical clinic users were computed by ten years age group was used as weighting coefficient for potential users of each medical clinic (demand).
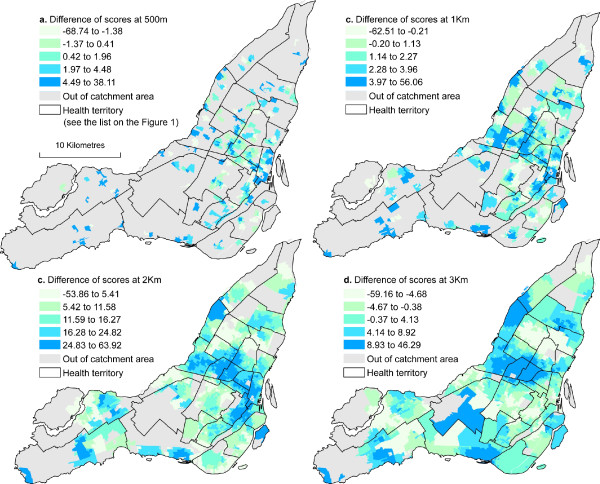
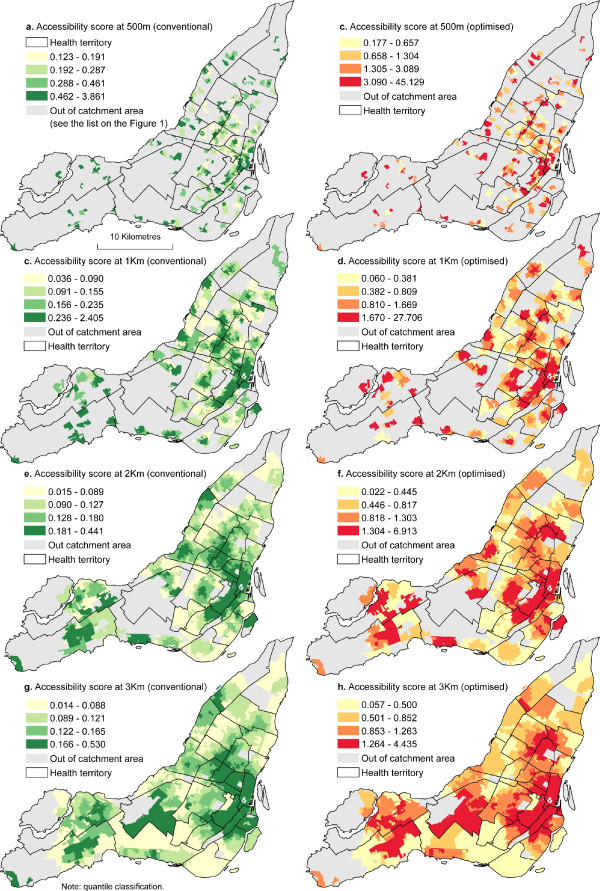
The spatial accessibility score (SA) increased considerably with the optimisation method. Within a distance of 1 Km, for instance, the maximum clinic accessible for 1,000 persons is 2.4 when the conventional method is used, compared with 27.7 for the optimized method. The t-test indicates a significant difference between the conventional and the optimized 2SFCA methods. Also, results of the differences between the two methods reveal a clustering of residuals when distance increases. In other words, a low threshold would be associated with a lack of precision.
Results of this study suggest that a greater effort must be made ameliorate spatial accessibility to medical clinics in Montreal. To ensure that health resources are allocated in the interest of the population, health planners and the government should consider a strategy in the sitting of future clinics which would provide spatial access to the greatest number of people.
减少医疗服务的空间可达性差距是医疗规划者日益关注的重点,尤其是在人口老龄化的发达国家。因此,迫切需要确定哪些人群无法获得医疗服务,但由于缺乏令人满意的衡量和方法,量化这种空间可达性差距的努力受到了阻碍。本研究比较了两步浮动捕获区(2SFCA)方法的优化版本和常规版本,以评估蒙特利尔医疗诊所的空间可达性。
我们首先根据最短网络距离计算了蒙特利尔岛现有医疗诊所的捕获区。传播区域内的人口用于确定给定医疗诊所的潜在使用者。为了优化该方法,我们对诊所(供应)进行了加权,权重为每个诊所工作的医生人数,而前一年的医疗诊所使用者则按十年年龄组进行计算,作为每个医疗诊所潜在使用者的权重系数(需求)。
空间可达性得分(SA)随着优化方法的使用而大幅提高。例如,在 1 公里的距离内,使用常规方法时,可容纳 1000 人的最大诊所数量为 2.4,而使用优化方法时则为 27.7。t 检验表明,常规 2SFCA 方法和优化 2SFCA 方法之间存在显著差异。此外,两种方法之间差异的结果表明,随着距离的增加,残差呈聚类分布。换句话说,低阈值将与精度不足相关。
本研究结果表明,必须加大力度改善蒙特利尔医疗诊所的空间可达性。为了确保卫生资源的分配符合人口利益,卫生规划者和政府应考虑在未来诊所的选址中采取一项策略,以便为最多的人提供空间可达性。