Centre Emergence, Institut Mutualiste Montsouris, Paris, France.
BMC Psychiatry. 2011 Jul 12;11:110. doi: 10.1186/1471-244X-11-110.
MDFT (Multidimensional Family Therapy) is a family based outpatient treatment programme for adolescent problem behaviour. MDFT has been found effective in the USA in adolescent samples differing in severity and treatment delivery settings. On request of five governments (Belgium, France, Germany, the Netherlands, and Switzerland), MDFT has now been tested in the joint INCANT trial (International Cannabis Need of Treatment) for applicability in Western Europe. In each of the five countries, study participants were recruited from the local population of youth seeking or guided to treatment for, among other things, cannabis use disorder. There is little information in the literature if these populations are comparable between sites/countries or not. Therefore, we examined if the study samples enrolled in the five countries differed in baseline characteristics regarding demographics, clinical profile, and treatment delivery setting.
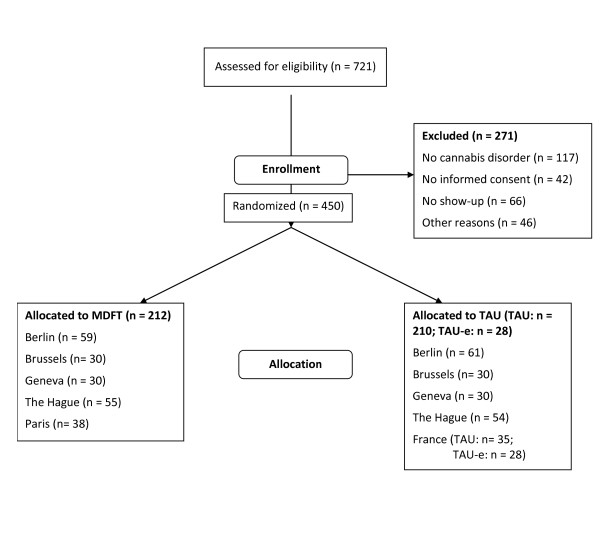
INCANT was a multicentre phase III(b) randomized controlled trial with an open-label, parallel group design. It compared MDFT with treatment as usual (TAU) at and across sites in Berlin, Brussels, Geneva, The Hague and Paris.Participants of INCANT were adolescents of either sex, from 13 through 18 years of age, with a cannabis use disorder (dependence or abuse), and at least one parent willing to take part in the treatment. In total, 450 cases/families were randomized (concealed) into INCANT.
We collected data about adolescent and family demographics (age, gender, family composition, school, work, friends, and leisure time). In addition, we gathered data about problem behaviour (substance use, alcohol and cannabis use disorders, delinquency, psychiatric co-morbidity).There were no major differences on any of these measures between the treatment conditions (MDFT and TAU) for any of the sites. However, there were cross-site differences on many variables. Most of these could be explained by variations in treatment culture, as reflected by referral policy, i.e., participants' referral source. We distinguished 'self-determined' referral (common in Brussels and Paris) and referral with some authority-related 'external' coercion (common in Geneva and The Hague). The two referral types were more equally divided in Berlin. Many cross-site baseline differences disappeared when we took referral source into account, but not all.
A multisite trial has the advantage of being efficient, but it also carries risks, the most important one being lack of equivalence between local study populations. Our site populations differed in many respects. This is not a problem for analyses and interpretations if the differences somehow can be accounted for. To a major extent, this appeared possible in INCANT. The most important factor underlying the cross-site variations in baseline characteristics was referral source. Correcting for referral source made most differences disappear. Therefore, we will use referral source as a covariate accounting for site differences in future INCANT outcome analyses.
ISRCTN: ISRCTN51014277.
MDFT(多维家庭治疗)是一种基于家庭的青少年问题行为门诊治疗方案。MDFT 已被证明在美国对不同严重程度和治疗提供环境的青少年样本有效。应五个政府(比利时、法国、德国、荷兰和瑞士)的要求,MDFT 现已在联合 INCANT 试验(国际大麻治疗需求)中进行了测试,以评估其在西欧的适用性。在这五个国家的每一个国家,研究参与者都是从当地寻求或被引导接受治疗的青少年人群中招募的,其中包括大麻使用障碍等问题。文献中关于这些人群在地点/国家之间是否可比的信息很少。因此,我们研究了五个国家的研究样本在人口统计学、临床特征和治疗提供环境方面是否存在差异。
INCANT 是一项多中心 III(b) 随机对照试验,采用开放标签、平行组设计。它比较了 MDFT 与柏林、布鲁塞尔、日内瓦、海牙和巴黎各地的常规治疗 (TAU)。INCANT 的参与者是年龄在 13 至 18 岁之间的任何性别的青少年,患有大麻使用障碍(依赖或滥用),并且至少有一位愿意参加治疗的父母。共有 450 例/家庭被随机(隐蔽)分配到 INCANT。
我们收集了关于青少年和家庭人口统计学(年龄、性别、家庭组成、学校、工作、朋友和休闲时间)的数据。此外,我们还收集了关于问题行为(药物使用、酒精和大麻使用障碍、犯罪、精神共病)的数据。对于任何地点,治疗条件(MDFT 和 TAU)之间在任何这些措施上都没有重大差异。然而,在许多变量上存在着跨地点的差异。这些差异中的大多数可以通过治疗文化的差异来解释,这反映在转诊政策上,即参与者的转诊来源。我们区分了“自我决定”的转诊(在布鲁塞尔和巴黎很常见)和带有一些权威相关的“外部”强制的转诊(在日内瓦和海牙很常见)。这两种转诊类型在柏林的分配更为平均。当我们考虑转诊来源时,许多跨地点的基线差异消失了,但并非全部。
多地点试验具有效率高的优点,但也存在风险,最重要的是当地研究人群之间缺乏等效性。我们的现场人群在许多方面存在差异。如果这些差异以某种方式可以得到解释,那么对于分析和解释来说,这不是一个问题。在很大程度上,INCANT 中似乎有可能。导致基线特征跨地点差异的最重要因素是转诊来源。通过校正转诊来源,大多数差异消失了。因此,我们将在未来的 INCANT 结果分析中使用转诊来源作为协变量来解释现场差异。
ISRCTN: ISRCTN51014277。