Singh Ranju, Arora Madhur, Vajifdar Homay
Associate Professor, Department of Anaesthesiology & Critical Care, Lady Hardinge Medical College & Associated Kalawati Saran Children's Hospital, New Delhi, India.
J Anaesthesiol Clin Pharmacol. 2011 Jan;27(1):91-6.
Till date, different combinations of adjuncts with induction agents have been tried for Laryngeal Mask Airway (LMA) insertion; yet, the ideal combination that provides the best insertion conditions with minimal side effects has not been identified, particularly in children. PATIENTS #ENTITYSTARTX00026;
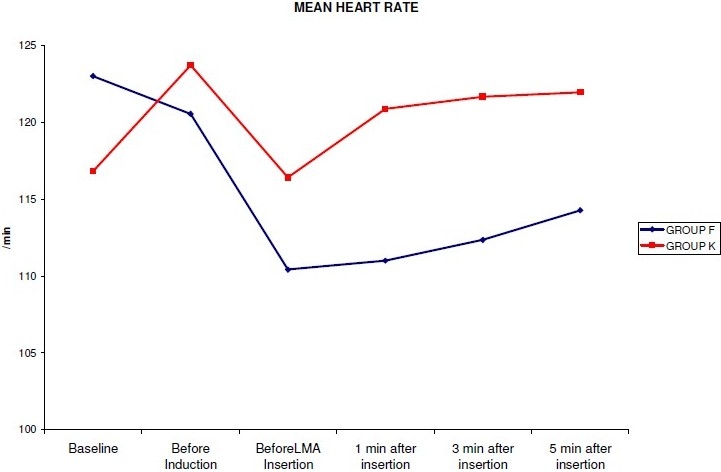
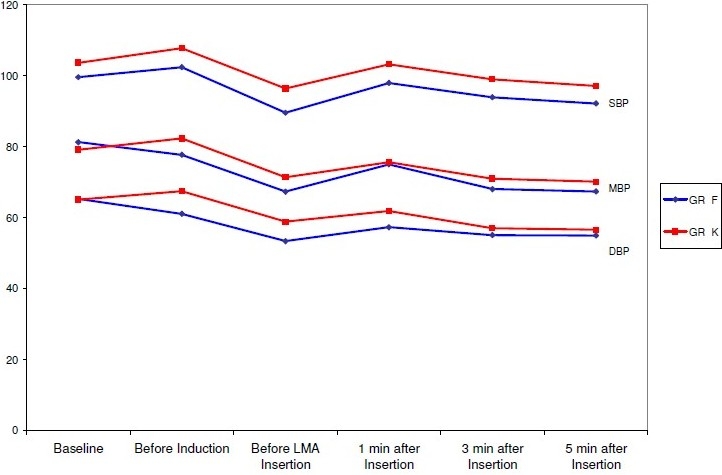
Hundred paediatric ASA grade I and II patients, aged 3-12 years, were randomly allocated to receive intravenously either fentanyl 2μg kg(-1) (Group F, n=50) or ketamine 0.5 mg kg(-1) (Group K, n=50), before induction of anaesthesia with propofol 3.5 mg kg(-1). Arterial blood pressure and heart rate were measured before induction (baseline), immediately before induction, immediately before LMA insertion, and at 1, 3 and 5 minutes after LMA insertion. Following LMA insertion, the following six subjective endpoints were graded by a blinded anaesthetist using ordinal scales graded 1 to 3: mouth opening, gagging, swallowing, head and limb movements, laryngospasm and resistance to insertion. Duration and incidence of apnoea was also recorded.
The incidence of resistance to mouth opening, resistance to LMA insertion and incidence of swallowing was not statistically significant between the two groups. Coughing/ gagging was seen in 8% patients in group K as compared to 28% patients in group K. Limb/ head movements were observed in 64% patients in the fentanyl group and in 76% patients in the ketamine group. Laryngospasm was not seen in any patient in either group. Incidence of apnoea was 80% in the fentanyl group and 50% in the ketamine group. The heart rate, systolic blood pressure, diastolic blood pressure and mean arterial pressure were consistently higher in the ketamine group as compared to the fentanyl group.
The combination of fentanyl (2μg kg-1) and propofol (3.5mg kg-1) provides better conditions for LMA insertion in children than a combination of ketamine (0.5 mg kg-1) and propofol (3.5mg kg-1).
迄今为止,人们尝试了多种诱导药物与辅助药物的不同组合用于喉罩置入;然而,尚未确定能提供最佳置入条件且副作用最小的理想组合,尤其是在儿童中。患者……
100例3至12岁的儿科ASA I级和II级患者,在使用3.5mg/kg丙泊酚进行麻醉诱导前,随机分为两组,分别静脉注射2μg/kg芬太尼(F组,n = 50)或0.5mg/kg氯胺酮(K组,n = 50)。在诱导前(基线)、诱导即刻、喉罩置入前即刻以及喉罩置入后1、3和5分钟测量动脉血压和心率。喉罩置入后,由一名不知情的麻醉医生使用分级为1至3的有序量表对以下六个主观终点进行评分:张口、恶心、吞咽、头部和肢体运动、喉痉挛和置入阻力。还记录了呼吸暂停的持续时间和发生率。
两组之间张口阻力、喉罩置入阻力和吞咽发生率无统计学差异。K组有8%的患者出现咳嗽/恶心,而F组为28%。芬太尼组64%的患者和氯胺酮组76%的患者观察到肢体/头部运动。两组均未观察到喉痉挛。芬太尼组呼吸暂停发生率为80%,氯胺酮组为50%。与芬太尼组相比,氯胺酮组的心率、收缩压、舒张压和平均动脉压持续较高。
与氯胺酮(0.5mg/kg)和丙泊酚(3.5mg/kg)的组合相比,芬太尼(2μg/kg)和丙泊酚(3.5mg/kg)的组合为儿童喉罩置入提供了更好的条件。