Kumar Sumit, Bajwa Sukhminder Jit Singh
Department of Anaesthesiology, Government Medical College, Patiala, India.
Saudi J Anaesth. 2011 Apr;5(2):142-9. doi: 10.4103/1658-354X.82781.
Neuraxial anesthesia in the elderly is associated with exaggerated responses to conventional doses of local anesthetics, thereby increasing the incidence of hemodynamic complications. A double-blind prospective study was carried out in our institute with an aim to compare the hemodynamic stability and quality of the conventional dose of hyperbaric bupivacaine (LA) with low dose of LA and sufentanil in elderly patients scheduled for lower limb surgery, randomized to receive combined spinal epidural anesthesia.
A total of 50 elderly patients of ASA grade I and II, divided randomly into groups I and II, of either sex undergoing lower limb surgery under combined spinal epidural anesthesia at our institute attached to a Government Medical College were enrolled for study. Group I received 2.5 ml of intrathecal hyperbaric bupivacaine (LA), while group II received 1.5 ml of intrathecal LA+0.1 ml sufentanil (5 μg). Both initial and postoperative subarachnoid block characteristics, hemodynamic and respiratory parameters, duration of analgesia, and side effects were observed and recorded. Statistical analysis was carried out using Chi-square and paired t test.
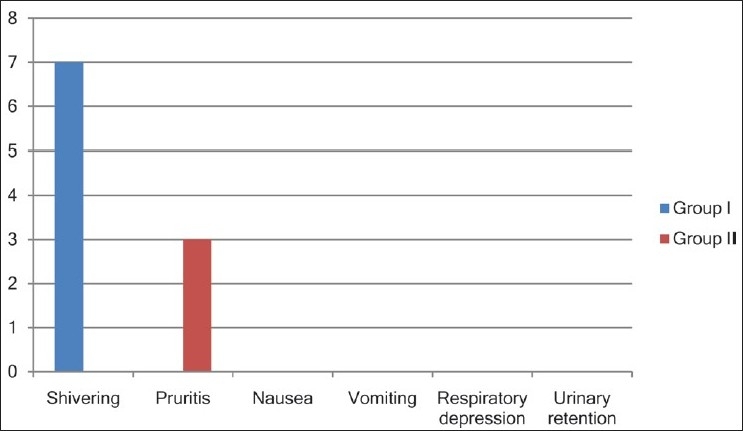
Demographic profile was comparable in both groups. Group I had a greater incidence of hypotension and, consequently, higher use of vasopressors (P<0.05). Onset of sensory analgesia, time to achieve peak sensory level, and recovery from motor blockade were significantly earlier in group II (P<0.05). Postoperative consumption of LA through epidural route was significantly higher in group I (P<0.05). The side effect profile was similar, except for a significantly higher incidence of shivering in group I (P<0.05).
The study established that the dose of a local anesthetic can be safely and significantly lowered by 40%, with addition of low-dose sufentanil, thereby avoiding the hemodynamic fluctuation and providing a stable perioperative and postoperative period in the geriatric population. In addition, duration of sensory analgesia is prolonged and postoperative requirement for the epidural top-up also decreases.
老年患者的椎管内麻醉与对常规剂量局部麻醉药的反应过度相关,从而增加了血流动力学并发症的发生率。我们研究所开展了一项双盲前瞻性研究,旨在比较常规剂量的重比重布比卡因(局部麻醉药)与低剂量局部麻醉药和舒芬太尼在计划进行下肢手术的老年患者中的血流动力学稳定性和质量,这些患者随机接受腰麻-硬膜外联合麻醉。
共有50例ASA I级和II级的老年患者,随机分为I组和II组,在一所隶属于政府医学院的研究所接受腰麻-硬膜外联合麻醉下的下肢手术,纳入研究。I组接受2.5 ml鞘内注射重比重布比卡因(局部麻醉药),而II组接受1.5 ml鞘内注射局部麻醉药+0.1 ml舒芬太尼(5μg)。观察并记录初始和术后蛛网膜下腔阻滞特征、血流动力学和呼吸参数、镇痛持续时间及副作用。采用卡方检验和配对t检验进行统计学分析。
两组的人口统计学特征具有可比性。I组低血压发生率更高,因此血管升压药的使用也更多(P<0.05)。II组感觉镇痛的起效时间、达到感觉峰值水平的时间和运动阻滞恢复时间明显更早(P<0.05)。I组术后通过硬膜外途径使用局部麻醉药的量明显更高(P<0.05)。除I组寒战发生率明显更高外(P<0.05),副作用情况相似。
该研究证实,加入低剂量舒芬太尼后,局部麻醉药的剂量可安全且显著降低40%,从而避免血流动力学波动,并为老年人群提供稳定的围手术期和术后阶段。此外,感觉镇痛的持续时间延长,术后硬膜外追加药物的需求也减少。