Brigham and Women's Hospital, Harvard Medical School, and Harvard School of Public Health, Boston, Massachusetts 02115, USA.
Ann Intern Med. 2011 Aug 2;155(3):160-70. doi: 10.7326/0003-4819-155-3-201108020-00006.
Few previous studies have evaluated associations between long-chain ω-3 fatty acids and incidence of congestive heart failure (CHF), and those that have are typically based on diet questionnaires and yield conflicting results. Circulating fatty acid concentrations provide objective biomarkers of exposure.
To determine whether plasma phospholipid concentrations of long-chain ω-3 fatty acids, including eicosapentaenoic acid (EPA), docosapentaenoic acid (DPA), and docosahexaenoic acid (DHA), were associated with incident CHF.
Prospective cohort study.
4 U.S. communities.
2735 U.S. adults without prevalent heart disease who were enrolled in the Cardiovascular Health Study from 1992 to 2006.
Plasma phospholipid fatty acid concentrations and other cardiovascular risk factors were measured in 1992 by using standardized methods. Relationships with incident CHF (555 cases during 26 490 person-years, adjudicated by using medical records) were assessed by using Cox proportional hazards models.
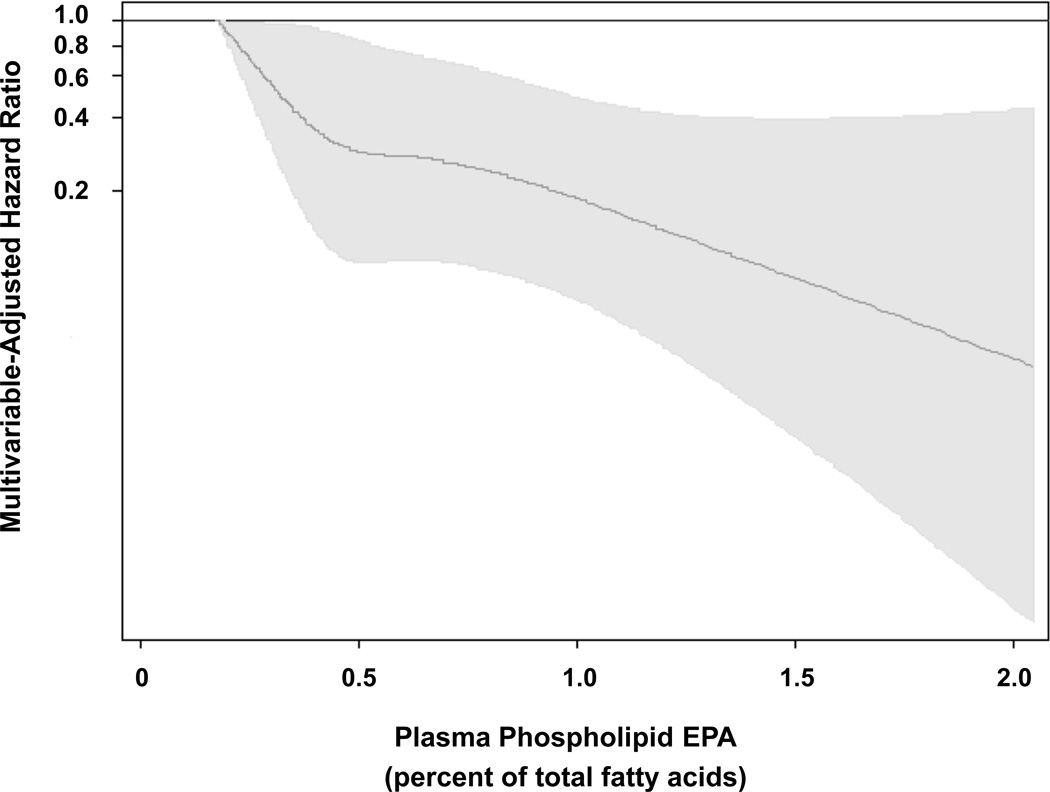
After multivariate adjustment, plasma phospholipid EPA concentration was inversely associated with incident CHF; risk was approximately 50% lower in the highest versus the lowest quartile (hazard ratio [HR], 0.52 [95% CI, 0.38 to 0.72]; P for trend = 0.001). In similar analyses, trends toward lower risk were seen for DPA (HR, 0.76 [CI, 0.56 to 1.04]; P for trend = 0.057) and total long-chain ω-3 fatty acids (HR, 0.70 [CI, 0.49 to 0.99]; P for trend = 0.062) but not for DHA (HR, 0.84 [CI, 0.58 to 1.21]; P for trend = 0.38). In analyses censored to the middle of follow-up (7 years) to minimize exposure misclassification over time, multivariate-adjusted HRs were 0.48 for EPA (CI, 0.32 to 0.71; P for trend = 0.005), 0.61 for DPA (CI, 0.39 to 0.95; P for trend = 0.033), 0.64 for DHA (CI, 0.40 to 1.04; P for trend = 0.057), and 0.51 for total ω-3 fatty acids (CI, 0.32 to 0.80; P for trend = 0.003).
Temporal changes in fatty acid concentrations over time may have caused underestimation of associations. Unmeasured or imperfectly measured covariates may have caused residual confounding.
Circulating individual and total ω-3 fatty acid concentrations are associated with lower incidence of CHF in older adults.
National Institutes of Health.
先前的研究很少评估长链 ω-3 脂肪酸与充血性心力衰竭(CHF)发病率之间的关联,而这些研究通常基于饮食问卷,得出的结果相互矛盾。循环脂肪酸浓度提供了暴露的客观生物标志物。
确定血浆磷脂长链 ω-3 脂肪酸(包括二十碳五烯酸(EPA)、二十二碳五烯酸(DPA)和二十二碳六烯酸(DHA))浓度是否与 CHF 的发生有关。
前瞻性队列研究。
美国 4 个社区。
1992 年至 2006 年期间参加心血管健康研究的 2735 名美国无明显心脏病的成年人。
通过标准化方法在 1992 年测量了血浆磷脂脂肪酸浓度和其他心血管风险因素。使用 Cox 比例风险模型评估与 CHF(555 例,26490 人年,通过病历进行裁决)发生的关系。
经过多变量调整后,血浆磷脂 EPA 浓度与 CHF 的发生呈负相关;最高四分位组与最低四分位组相比,风险降低约 50%(风险比 [HR],0.52 [95%CI,0.38 至 0.72];趋势 P 值=0.001)。在类似的分析中,DPA(HR,0.76 [CI,0.56 至 1.04];趋势 P 值=0.057)和总长链 ω-3 脂肪酸(HR,0.70 [CI,0.49 至 0.99];趋势 P 值=0.062)的风险呈下降趋势,但 DHA 无此趋势(HR,0.84 [CI,0.58 至 1.21];趋势 P 值=0.38)。在随访中期(7 年)进行的分析中,对时间相关的暴露分类错误进行了删截,以最大程度地减少,EPA 的多变量调整 HR 为 0.48(CI,0.32 至 0.71;趋势 P 值=0.005),DPA 为 0.61(CI,0.39 至 0.95;趋势 P 值=0.033),DHA 为 0.64(CI,0.40 至 1.04;趋势 P 值=0.057),总 ω-3 脂肪酸为 0.51(CI,0.32 至 0.80;趋势 P 值=0.003)。
随着时间的推移,脂肪酸浓度的时间变化可能导致关联的低估。未测量或测量不完全的协变量可能导致残留混杂。
年长成年人循环的个体和总 ω-3 脂肪酸浓度与 CHF 的发病率较低有关。
美国国立卫生研究院。