University of Pittsburgh, Pittsburgh, Pennsylvania, United States of America.
PLoS One. 2011;6(9):e24673. doi: 10.1371/journal.pone.0024673. Epub 2011 Sep 13.
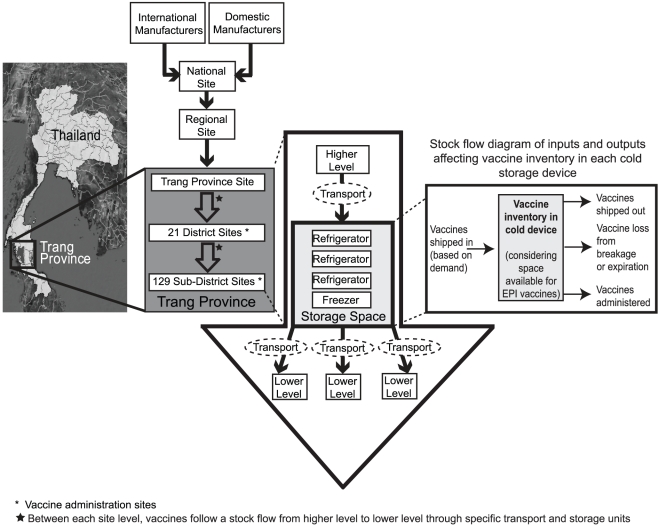
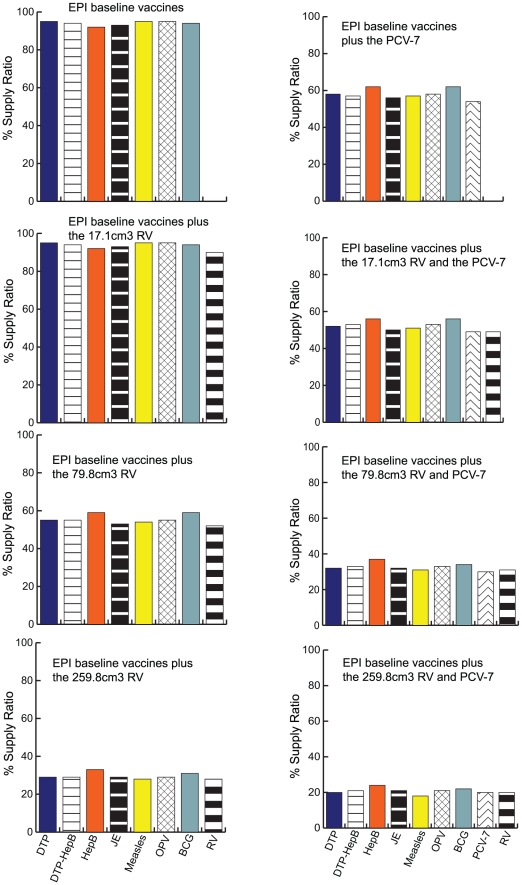
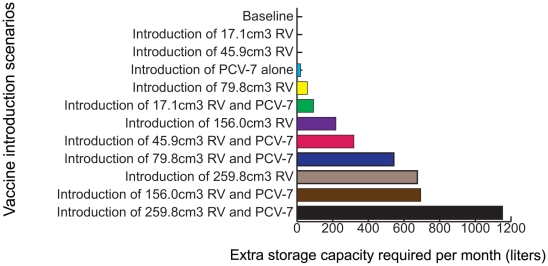
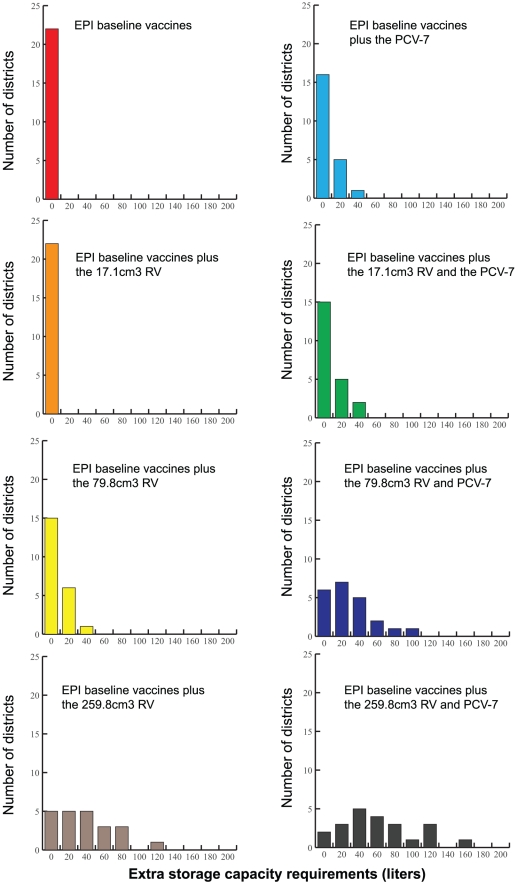
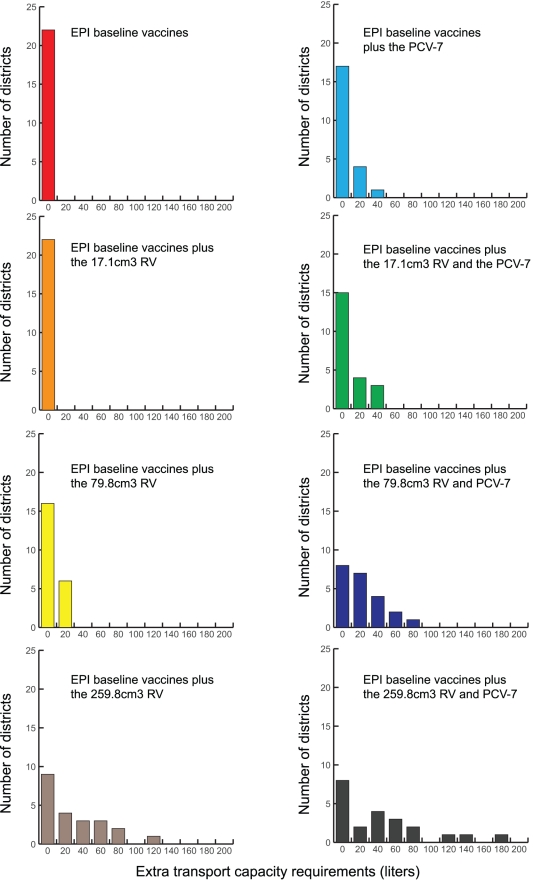
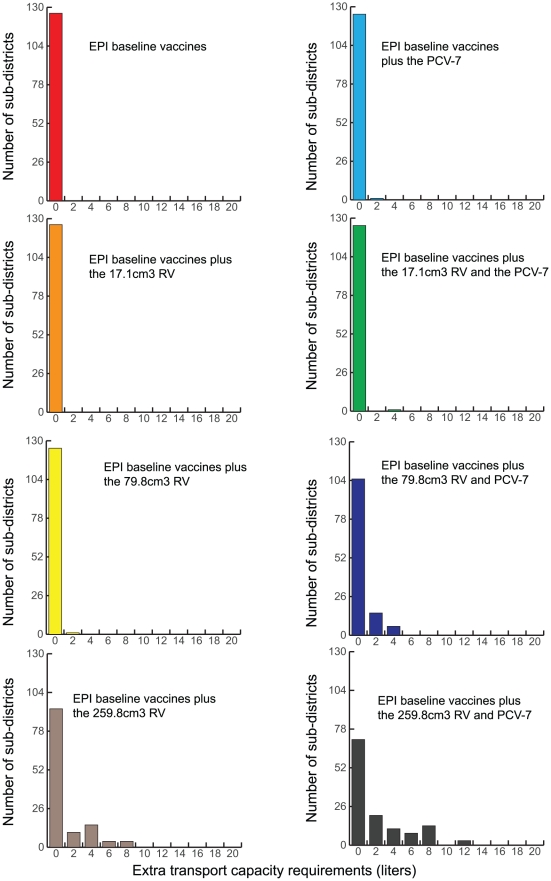
Although the substantial burdens of rotavirus and pneumococcal disease have motivated many countries to consider introducing the rotavirus vaccine (RV) and heptavalent pneumococcal conjugate vaccine (PCV-7) to their National Immunization Programs (EPIs), these new vaccines could affect the countries' vaccine supply chains (i.e., the series of steps required to get a vaccine from their manufacturers to patients). We developed detailed computational models of the Trang Province, Thailand, vaccine supply chain to simulate introducing various RV and PCV-7 vaccine presentations and their combinations. Our results showed that the volumes of these new vaccines in addition to current routine vaccines could meet and even exceed (1) the refrigerator space at the provincial district and sub-district levels and (2) the transport cold space at district and sub-district levels preventing other vaccines from being available to patients who arrive to be immunized. Besides the smallest RV presentation (17.1 cm³/dose), all other vaccine introduction scenarios required added storage capacity at the provincial level (range: 20 L-1151 L per month) for the three largest formulations, and district level (range: 1 L-124 L per month) across all introduction scenarios. Similarly, with the exception of the two smallest RV presentation (17.1 cm³/dose), added transport capacity was required at both district and sub-district levels. Added transport capacity required across introduction scenarios from the provincial to district levels ranged from 1 L-187 L, and district to sub-district levels ranged from 1 L-13 L per shipment. Finally, only the smallest RV vaccine presentation (17.1 cm³/dose) had no appreciable effect on vaccine availability at sub-districts. All other RV and PCV-7 vaccines were too large for the current supply chain to handle without modifications such as increasing storage or transport capacity. Introducing these new vaccines to Thailand could have dynamic effects on the availability of all vaccines that may not be initially apparent to decision-makers.
虽然轮状病毒和肺炎球菌疾病的巨大负担促使许多国家考虑在国家免疫规划(EPI)中引入轮状病毒疫苗(RV)和七价肺炎球菌结合疫苗(PCV-7),但这些新疫苗可能会影响国家的疫苗供应链(即从制造商到患者获得疫苗所需的一系列步骤)。我们开发了泰国桐艾府疫苗供应链的详细计算模型,以模拟引入各种 RV 和 PCV-7 疫苗产品及其组合。结果表明,除了当前常规疫苗外,这些新疫苗的数量可以满足甚至超过(1)省和县一级的冰箱空间,(2)区和县一级的运输冷藏空间,从而防止其他疫苗可供前来接种的患者使用。除了最小的 RV 产品(17.1cm³/剂)外,所有其他疫苗引入方案都需要在省级(范围:每月 20-1151L)和区级(范围:每月 1-124L)增加存储容量,适用于所有引入方案。同样,除了两个最小的 RV 产品(17.1cm³/剂)外,还需要在区和县一级增加运输能力。从省级到区级的所有引入方案所需的额外运输能力范围从 1-187L,从区到县级的范围从 1-13L/批。最后,只有最小的 RV 疫苗产品(17.1cm³/剂)对县级以下的疫苗供应没有明显影响。所有其他 RV 和 PCV-7 疫苗都太大,目前的供应链无法处理,除非增加存储或运输能力等进行修改。将这些新疫苗引入泰国可能会对所有疫苗的供应产生动态影响,而这些影响最初可能不会被决策者察觉。