Center for Global Health and Diseases, Case Western Reserve University School of Medicine, Cleveland, Ohio, USA.
PLoS Negl Trop Dis. 2011 Sep;5(9):e1321. doi: 10.1371/journal.pntd.0001321. Epub 2011 Sep 20.
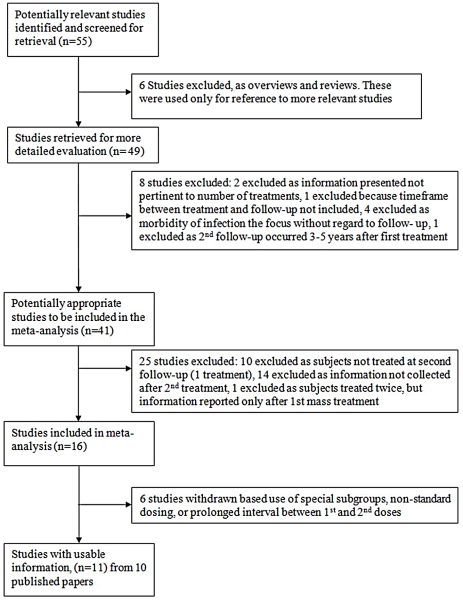
Controversy persists about the optimal approach to drug-based control of schistosomiasis in high-risk communities. In a systematic review of published studies, we examined evidence for incremental benefits from repeated praziquantel dosing, given 2 to 8 weeks after an initial dose, in Schistosoma-endemic areas of Africa.
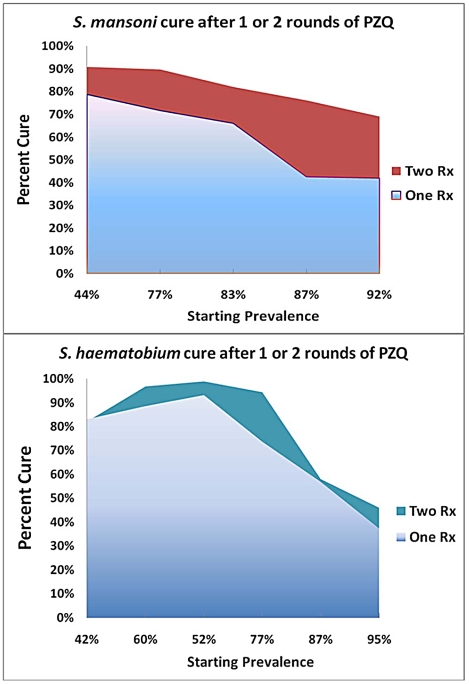
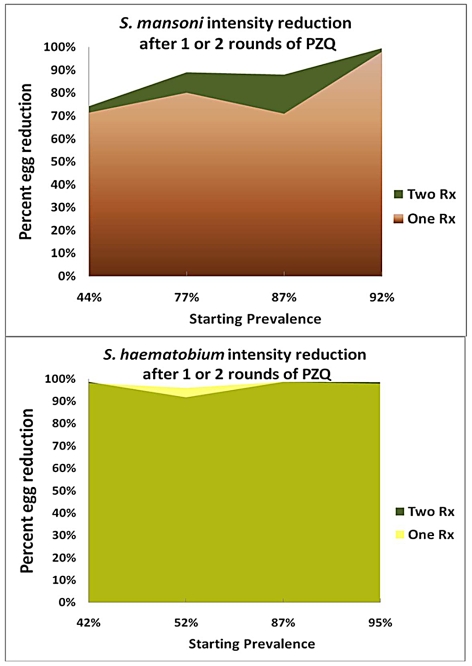
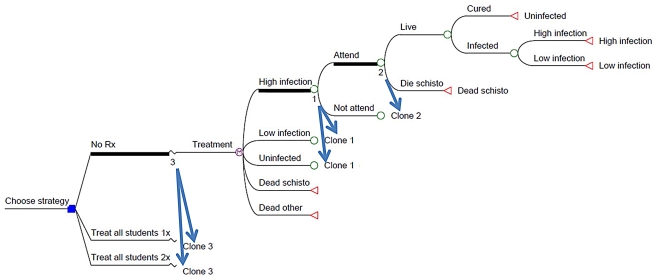
METHODOLOGY/PRINCIPAL FINDINGS: We performed systematic searches of electronic databases PubMed and EMBASE for relevant data using search terms 'schistosomiasis', 'dosing' and 'praziquantel' and hand searches of personal collections and bibliographies of recovered articles. In 10 reports meeting study criteria, improvements in parasitological treatment outcomes after two doses of praziquantel were greater for S. mansoni infection than for S. haematobium infection. Observed cure rates (positive to negative conversion in egg detection assays) were, for S. mansoni, 69-91% cure after two doses vs. 42-79% after one dose and, for S. haematobium, 46-99% cure after two doses vs. 37-93% after a single dose. Treatment benefits in terms of reduction in intensity (mean egg count) were also different for the two species-for S. mansoni, the 2-dose regimen yielded an weighted average 89% reduction in standardized egg counts compared to a 83% reduction after one dose; for S. haematobium, two doses gave a 93% reduction compared to a 94% reduction with a single dose. Cost-effectiveness analysis was performed based on Markov life path modeling.
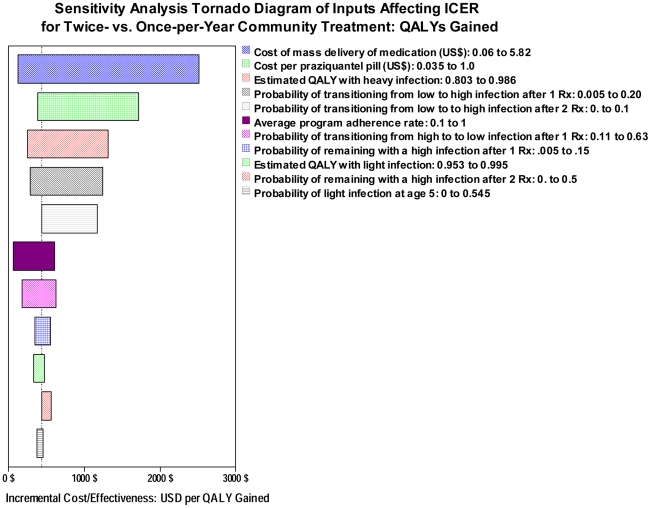
CONCLUSIONS/SIGNIFICANCE: Although schedules for repeated treatment with praziquantel require greater inputs in terms of direct costs and community participation, there are incremental benefits to this approach at an estimated cost of $153 (S. mansoni)-$211 (S. haematobium) per additional lifetime QALY gained by double treatment in school-based programs. More rapid reduction of infection-related disease may improve program adherence, and if, as an externality of the program, transmission can be reduced through more effective coverage, significant additional benefits are expected to accrue in the targeted communities.
在高风险社区中,针对血吸虫病的药物控制方法,仍存在争议。在对非洲血吸虫病流行地区发表的研究进行系统评价中,我们评估了在初始剂量后 2 至 8 周重复给予吡喹酮治疗的增量效益的证据。
方法/主要发现:我们使用“schistosomiasis”、“dosing”和“praziquantel”等搜索词,在电子数据库 PubMed 和 EMBASE 中进行了系统搜索,并检索了已检索文章的个人收藏和参考文献的手检,以获取相关数据。在符合研究标准的 10 份报告中,对于 S. mansoni 感染,两剂吡喹酮治疗后的寄生虫学治疗结局改善大于 S. haematobium 感染。观察到的治愈率(在卵检测试验中从阳性转为阴性)分别为:两剂后 S. mansoni 为 69-91%,一剂后为 42-79%;两剂后 S. haematobium 为 46-99%,一剂后为 37-93%。两种物种的强度(平均卵计数)降低方面的治疗效益也不同-对于 S. mansoni,两剂方案使标准化卵计数的加权平均降低了 89%,而一剂则降低了 83%;对于 S. haematobium,两剂降低了 93%,而一剂降低了 94%。基于马尔可夫生命路径建模进行了成本效益分析。
结论/意义:尽管重复使用吡喹酮治疗的方案在直接成本和社区参与方面需要更多的投入,但在以学校为基础的方案中,双治疗可获得额外的终生 QALY(质量调整生命年)收益,估计成本为 153 美元(S. mansoni)-211 美元(S. haematobium)。更快地降低与感染相关的疾病可能会提高方案的依从性,如果作为方案的外在因素,通过更有效的覆盖范围可以减少传播,那么目标社区预计会获得额外的显著收益。