Reese Rebecca L, Freedland Kenneth E, Steinmeyer Brian C, Rich Michael W, Rackley Justin W, Carney Robert M
Department of Psychology, Department of Psychiatry, and Department of Medicine, Washington University School of Medicine, 4320 Forest Park Avenue, St Louis, MO 63108, USA.
Circ Cardiovasc Qual Outcomes. 2011 Nov 1;4(6):626-33. doi: 10.1161/CIRCOUTCOMES.111.961896. Epub 2011 Oct 18.
Elevated scores on depression symptom questionnaires predict rehospitalization after acute myocardial infarction (AMI). Whether the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, depressive disorders predict rehospitalization after AMI is unknown.
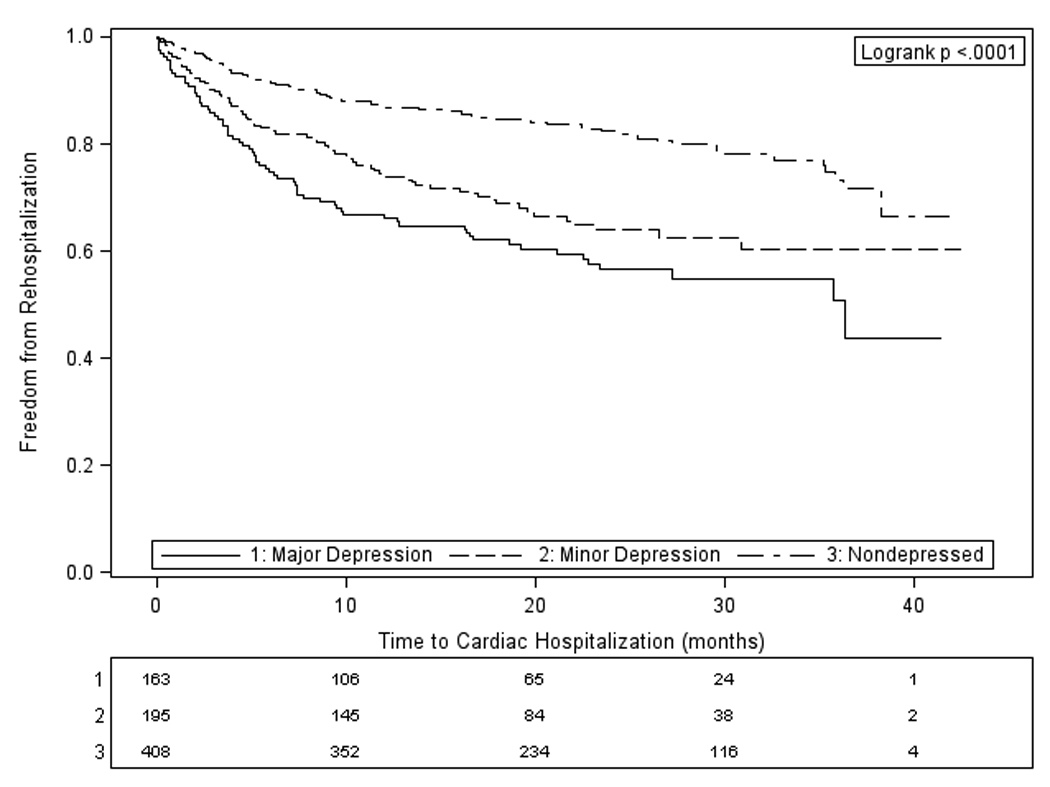
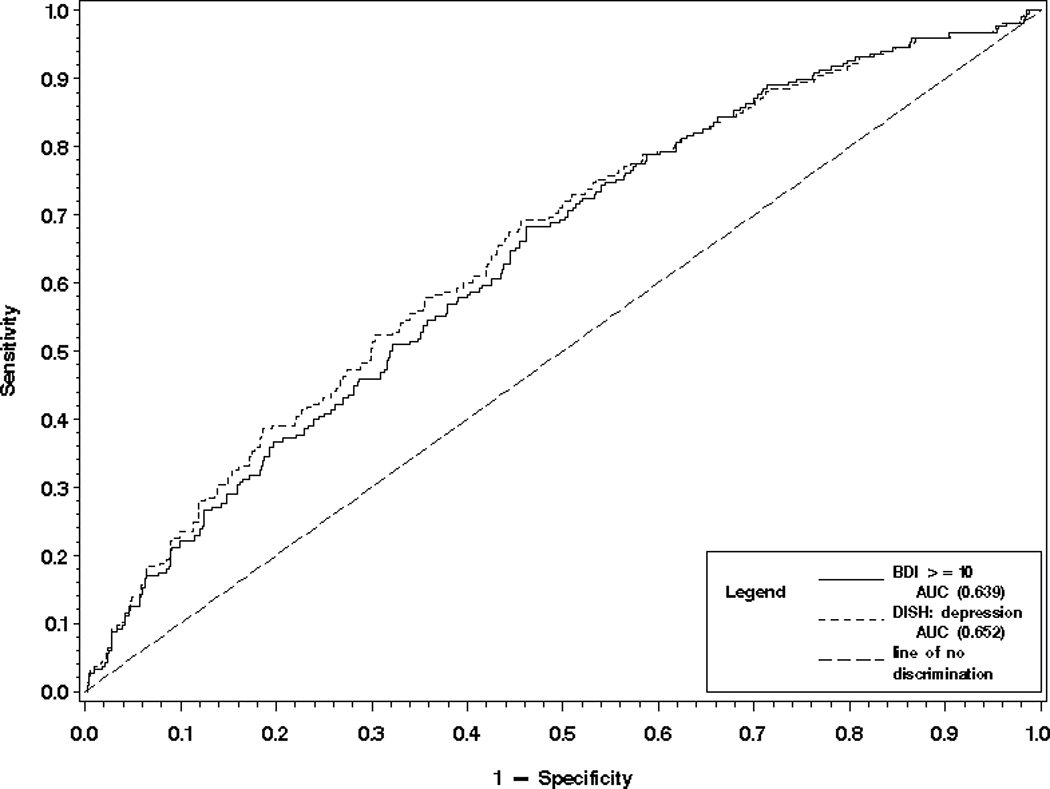
Participants (n=766) in an Enhancing Recovery and Coronary Heart Disease ancillary study were classified by diagnostic interview as having no depression, minor depression, or major depression after AMI. Cardiac rehospitalizations were tracked for up to 42 months. Cox proportional hazards regression was used to model the effect of depressive disorder on time to first cardiac rehospitalization, controlling for mortality risk factors. Logistic regression was used to compare the accuracy with which rehospitalization could be predicted by depression diagnosis or by the Beck Depression Inventory (BDI). Secondary analyses examined the effects of depression on the cumulative number of all-cause rehospitalizations, length of stay, and emergency department visits. Compared with patients without depression, patients with either minor or major depression were hospitalized sooner (minor depression adjusted hazard ratio, 2.22; 95% CI, 1.59-3.08; P<0.001; major depression adjusted hazard ratio, 2.54; 95% CI, 1.84-3.53; P<0.001), had more hospitalizations (minor, P<0.001; major, P<0.001) and emergency department visits (minor, P=0.003; major, P<0.001), and spent more days in the hospital (minor, P<0.001; major, P<0.001). The interview and questionnaire methods of assessing depression did not significantly differ in their overall accuracy of predicting rehospitalization.
Depressive disorders increase the risk of rehospitalization after AMI. Future work should focus on developing multivariable models to predict risk of rehospitalization after AMI, and depression should be included in these.
抑郁症状问卷得分升高可预测急性心肌梗死(AMI)后的再住院情况。《精神疾病诊断与统计手册》第四版中的抑郁障碍是否能预测AMI后的再住院情况尚不清楚。
在一项“强化康复与冠心病”辅助研究中,766名参与者通过诊断性访谈被分类为AMI后无抑郁、轻度抑郁或重度抑郁。对心脏再住院情况进行了长达42个月的跟踪。采用Cox比例风险回归模型来模拟抑郁障碍对首次心脏再住院时间的影响,并对死亡风险因素进行控制。采用逻辑回归来比较抑郁诊断或贝克抑郁量表(BDI)预测再住院的准确性。二次分析研究了抑郁对全因再住院累计次数、住院时间和急诊就诊次数的影响。与无抑郁的患者相比,轻度或重度抑郁患者更早住院(轻度抑郁调整风险比为2.22;95%CI为1.59 - 3.08;P<0.001;重度抑郁调整风险比为2.54;95%CI为1.84 - 3.53;P<0.001),住院次数更多(轻度,P<0.001;重度,P<0.001)和急诊就诊次数更多(轻度,P = 0.003;重度,P<0.001),且住院天数更长(轻度,P<0.001;重度,P<0.001)。评估抑郁的访谈法和问卷法在预测再住院的总体准确性上没有显著差异。
抑郁障碍会增加AMI后再住院的风险。未来的工作应侧重于开发多变量模型来预测AMI后的再住院风险,且应将抑郁纳入其中。