Dietz Noella A, Sherman Recinda, Mackinnon Jill, Fleming Lora, Arheart Kristopher L, Wohler Brad, Lee David J
Department of Epidemiology and Public Health, Sylvester Comprehensive Cancer Center, University of Miami Miller School of Medicine.
J Carcinog. 2011;10:22. doi: 10.4103/1477-3163.85184. Epub 2011 Sep 21.
Smoking-attributable risks for lung, esophageal, and head and neck (H/N) cancers range from 54% to 90%. Identifying areas with higher than average cancer risk and smoking rates, then targeting those areas for intervention, is one approach to more rapidly lower the overall tobacco disease burden in a given state. Our research team used spatial modeling techniques to identify areas in Florida with higher than expected tobacco-associated cancer incidence clusters.
Geocoded tobacco-associated incident cancer data from 1998 to 2002 from the Florida Cancer Data System were used. Tobacco-associated cancers included lung, esophageal, and H/N cancers. SaTScan was used to identify geographic areas that had statistically significant (P<0.10) excess age-adjusted rates of tobacco-associated cancers. The Poisson-based spatial scan statistic was used. Phi correlation coefficients were computed to examine associations among block groups with/without overlapping cancer clusters. The logistic regression was used to assess associations between county-level smoking prevalence rates and being diagnosed within versus outside a cancer cluster. Community-level smoking rates were obtained from the 2002 Florida Behavioral Risk Factor Surveillance System (BRFSS). Analyses were repeated using 2007 BRFSS to examine the consistency of associations.
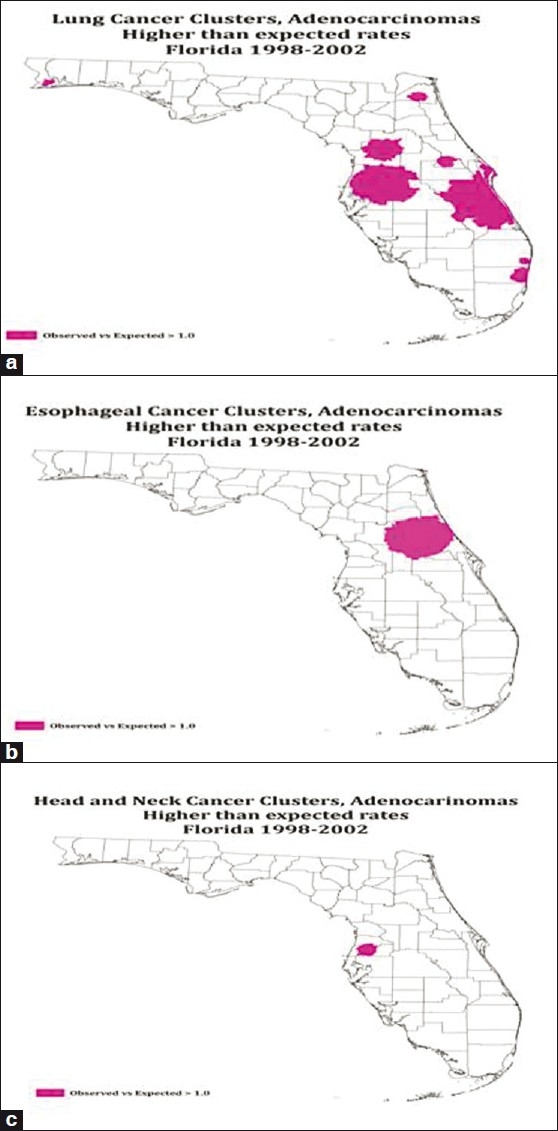
Lung cancer clusters were geographically larger for both squamous cell and adenocarcinoma cases in Florida from 1998 to 2002, than esophageal or H/N clusters. There were very few squamous cell and adenocarcinoma esophageal cancer clusters. H/N cancer mapping showed some squamous cell and a very small amount of adenocarcinoma cancer clusters. Phi correlations were generally weak to moderate in strength. The odds of having an invasive lung cancer cluster increased by 12% per increase in the county-level smoking rate. Results were inconsistent for esophageal and H/N cancers, with some inverse associations. 2007 BRFSS data also showed a similar results pattern.
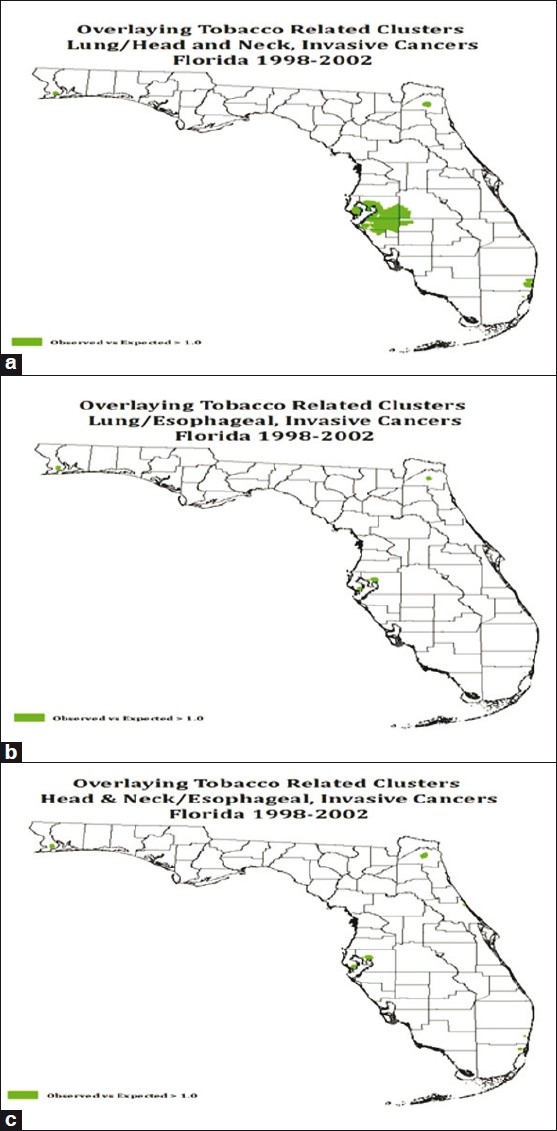
Spatial analysis identified many nonoverlapping areas of high risk across both cancer and histological subtypes. Attempts to correlate county-level smoking rates with cancer cluster membership yielded consistent results only for lung cancer. However, spatial analyses may be most useful when examining incident clusters where several tobacco-associated cancer clusters overlap. Focusing on overlapping cancer clusters may help investigators identify priority areas for further screening, detailed assessments of tobacco use, and/or prevention and cessation interventions to decrease risk.
吸烟导致肺癌、食管癌以及头颈癌的风险在54%至90%之间。识别癌症风险和吸烟率高于平均水平的地区,然后针对这些地区进行干预,是在特定州更快降低总体烟草疾病负担的一种方法。我们的研究团队使用空间建模技术来识别佛罗里达州中与烟草相关的癌症发病率高于预期的地区。
使用了来自佛罗里达癌症数据系统的1998年至2002年地理编码的与烟草相关的癌症发病数据。与烟草相关的癌症包括肺癌、食管癌以及头颈癌。空间扫描统计软件(SaTScan)用于识别年龄调整后的与烟草相关癌症发病率在统计学上显著过高(P<0.10)的地理区域。使用了基于泊松分布的空间扫描统计量。计算了Phi相关系数,以检验有/无重叠癌症聚集的街区组之间的关联。使用逻辑回归来评估县级吸烟流行率与在癌症聚集区内或外被诊断之间的关联。社区层面的吸烟率来自2002年佛罗里达行为风险因素监测系统(BRFSS)。使用2007年BRFSS重复分析以检验关联的一致性。
1998年至2002年,佛罗里达州鳞状细胞癌和腺癌病例的肺癌聚集区在地理上比食管癌或头颈癌聚集区更大。鳞状细胞癌和腺癌食管癌聚集区很少。头颈癌图谱显示了一些鳞状细胞癌聚集区和极少量腺癌聚集区。Phi相关性强度一般较弱至中等。县级吸烟率每增加1%,发生侵袭性肺癌聚集的几率增加12%。食管癌和头颈癌的结果不一致,存在一些负相关。2007年BRFSS数据也显示了类似的结果模式。
空间分析识别出了癌症和组织学亚型中许多不重叠的高风险区域。将县级吸烟率与癌症聚集区成员进行关联的尝试仅在肺癌方面产生了一致的结果。然而,在检查多个与烟草相关的癌症聚集区重叠的发病聚集区时,空间分析可能最有用。关注重叠的癌症聚集区可能有助于研究人员确定进一步筛查、详细评估烟草使用和/或预防及戒烟干预以降低风险的优先区域。