Anesthesiology and Intensive Care Unit, Hôtel Dieu Nantes University Hospital, 1 place Alexis Ricordeau, Nantes, F-44093 France.
Crit Care. 2011;15(5):R260. doi: 10.1186/cc10522. Epub 2011 Oct 28.
Description of a continuous hypertonic saline solution (HSS) infusion using a dose-adaptation of natremia in traumatic brain injured (TBI) patients with refractory intracranial hypertension (ICH).
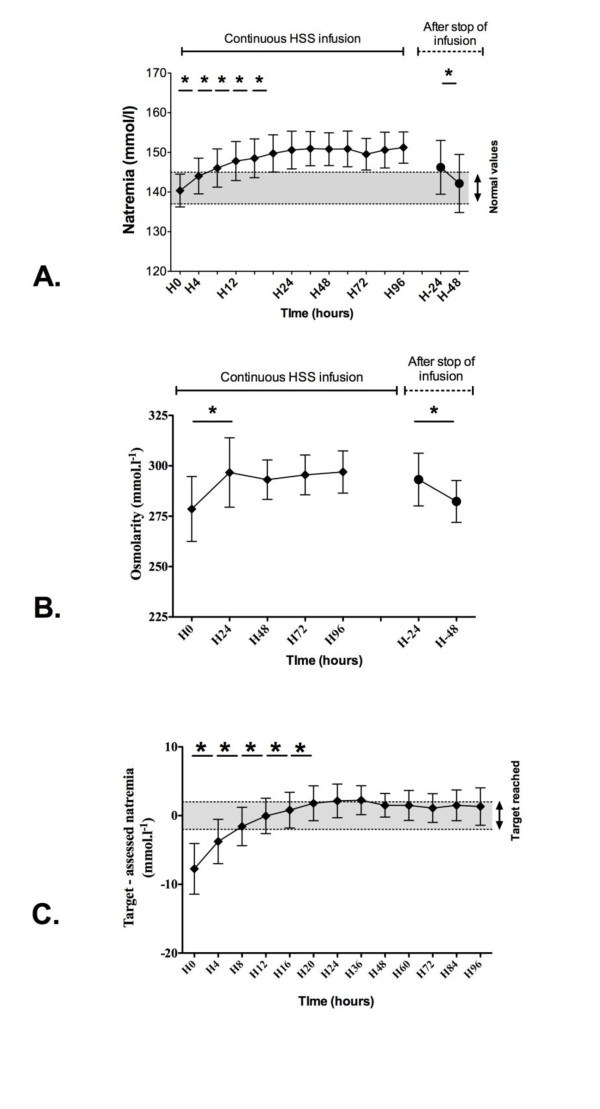
We performed a single-center retrospective study in a surgical intensive care unit of a tertiary hospital. Fifty consecutive TBI patients with refractory ICH treated with continuous HSS infusion adapted to a target of natremia. In brief, a physician set a target of natremia adapted to the evolution of intracranial pressure (ICP). Flow of NaCl 20% was a priori calculated according to natriuresis, and the current and target natremia that were assessed every 4 hours.
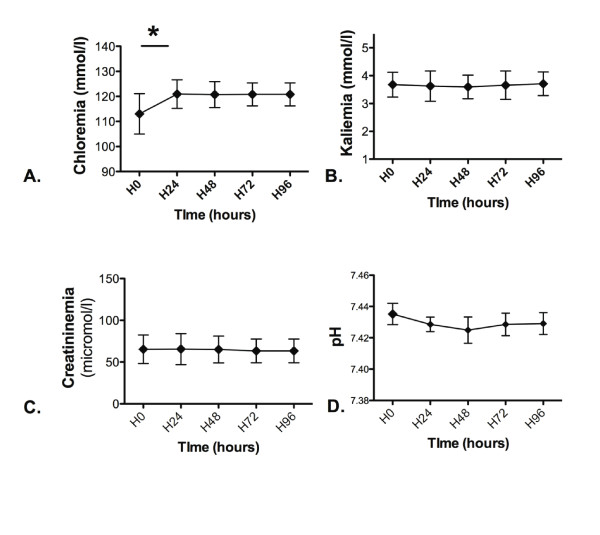
The HSS infusion was initiated for a duration of 7 (5 to 10) (8 ± 4) days. ICP decreased from 29 (26 to 34) (31 ± 9) mm Hg at H0 to 20 (15 to 26) (21 ± 8) mm Hg at H1 (P < 0.05). Cerebral perfusion pressure increased from 61 (50 to 70) (61 ± 13) mm Hg at H0 up to 67 (60 to 79) (69 ± 12) mm Hg at H1 (P < 0.05). No rebound of ICH was reported after stopping continuous HSS infusion. Natremia increased from 140 (138 to 143) (140 ± 4) at H0 up to 144 (141 to 148) (144 ± 4) mmol/L at H4 (P < 0.05). Plasma osmolarity increased from 275 (268 to 281) (279 ± 17) mmol/L at H0 up to 290 (284 to 307) (297 ± 17) mmol/L at H24 (P < 0.05). The main side effect observed was an increase in chloremia from 111 (107 to 119) (113 ± 8) mmol/L at H0 up to 121 (117 to 124) (121 ± 6) mmol/L at H24 (P < 0.05). Neither acute kidney injury nor pontine myelinolysis was recorded.
Continuous HSS infusion adapted to close biologic monitoring enables long-lasting control of natremia in TBI patients along with a decreased ICP without any rebound on infusion discontinuation.
描述了一种连续高渗盐水溶液(HSS)输注方法,该方法通过适应创伤性脑损伤(TBI)患者颅内压升高(ICH)的血钠来进行剂量调整。
我们在一家三级医院的外科重症监护病房进行了一项单中心回顾性研究。50 例连续 TBI 患者因难治性 ICH 接受了连续 HSS 输注,该输注方法适应血钠的目标值。简而言之,医生设定了适应颅内压(ICP)演变的血钠目标值。根据尿钠排泄量预先计算了 20%NaCl 的流速,并且每 4 小时评估当前和目标血钠值。
HSS 输注持续了 7(5 至 10)(8 ± 4)天。ICP 从 H0 时的 29(26 至 34)(31 ± 9)mmHg 降至 H1 时的 20(15 至 26)(21 ± 8)mmHg(P < 0.05)。脑灌注压从 H0 时的 61(50 至 70)(61 ± 13)mmHg 增加至 H1 时的 67(60 至 79)(69 ± 12)mmHg(P < 0.05)。停止连续 HSS 输注后,未报告 ICH 反弹。血钠从 H0 时的 140(138 至 143)(140 ± 4)mmol/L 增加至 H4 时的 144(141 至 148)(144 ± 4)mmol/L(P < 0.05)。血浆渗透压从 H0 时的 275(268 至 281)(279 ± 17)mmol/L 增加至 H24 时的 290(284 至 307)(297 ± 17)mmol/L(P < 0.05)。观察到的主要副作用是氯血症增加,从 H0 时的 111(107 至 119)(113 ± 8)mmol/L 增加至 H24 时的 121(117 至 124)(121 ± 6)mmol/L(P < 0.05)。未记录到急性肾损伤或脑桥髓鞘溶解。
连续 HSS 输注适应生物监测,可使 TBI 患者的血钠得到长期控制,ICP 降低,并且在停止输注时不会出现反弹。