Institute for Clinical Pharmacology, Hannover Medical School, Hannover, Germany.
PLoS One. 2011;6(10):e26489. doi: 10.1371/journal.pone.0026489. Epub 2011 Oct 25.
Due to lack of efficacy in recent trials, current guidelines for the treatment of neurally-mediated (vasovagal) syncope do not promote cardiac pacemaker implantation. However, the finding of asystole during head-up tilt -induced (pre)syncope may lead to excessive cardioinhibitory syncope diagnosis and treatment with cardiac pacemakers as blood pressure is often discontinuously measured. Furthermore, physicians may be more inclined to implant cardiac pacemakers in older patients. We hypothesized that true cardioinhibitory syncope in which the decrease in heart rate precedes the fall in blood pressure is a very rare finding which might explain the lack of efficacy of pacemakers in neurally-mediated syncope.
We studied 173 consecutive patients referred for unexplained syncope (114 women, 59 men, 42 ± 1 years, 17 ± 2 syncopal episodes). All had experienced (pre)syncope during head-up tilt testing followed by additional lower body negative suction. We classified hemodynamic responses according to the modified Vasovagal Syncope International Study (VASIS) classification as mixed response (VASIS I), cardioinhibitory without (VASIS IIa) or with asystole (VASIS IIb), and vasodepressor (VASIS III). Then, we defined the exact temporal relationship between hypotension and bradycardia to identify patients with true cardioinhibitory syncope.
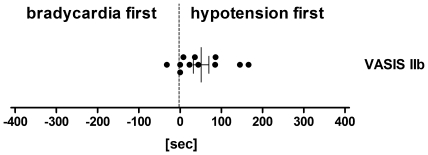
Of the (pre)syncopal events during tilt testing, 63% were classified as VASIS I, 6% as VASIS IIb, 2% as VASIS IIa, and 29% as VASIS III. Cardioinhibitory responses (VASIS class II) progressively decreased from the youngest to the oldest age quartile. With more detailed temporal analysis, blood pressure reduction preceded the heart-rate decrease in all but six individuals (97%) overall and in 10 out of 11 patients with asystole (VASIS IIb).
Hypotension precedes bradycardia onset during head-up tilt-induced (pre)syncope in the vast majority of patients, even in those classified as cardioinhibitory syncope according to the modified VASIS classification. Furthermore, cardioinhibitory syncope becomes less frequent with increasing age.
由于近期试验疗效不佳,目前治疗神经介导(血管迷走性)晕厥的指南不提倡植入心脏起搏器。然而,在头高位倾斜诱发(预)晕厥期间发现停搏可能导致过度的心抑制性晕厥诊断和治疗,因为血压通常是不连续测量的。此外,医生可能更倾向于在老年患者中植入心脏起搏器。我们假设,真正的心抑制性晕厥中,心率的下降先于血压的下降,这是一种非常罕见的发现,这可能解释了神经介导性晕厥中起搏器疗效不佳的原因。
我们研究了 173 例因不明原因晕厥而就诊的连续患者(114 例女性,59 例男性,42±1 岁,17±2 次晕厥发作)。所有患者在头高位倾斜试验中均经历过(预)晕厥,随后进行了额外的下体负压抽吸。我们根据改良的血管迷走性晕厥国际研究(VASIS)分类将血流动力学反应分类为混合反应(VASIS I)、无(VASIS IIa)或伴有停搏的心脏抑制(VASIS IIb)以及血管抑制性(VASIS III)。然后,我们确定了低血压和心动过缓之间的确切时间关系,以确定真正的心抑制性晕厥患者。
在倾斜试验中的(预)晕厥事件中,63%被归类为 VASIS I,6%归类为 VASIS IIb,2%归类为 VASIS IIa,29%归类为 VASIS III。心脏抑制反应(VASIS 类 II)从最年轻到最年长的四分位数逐渐减少。通过更详细的时间分析,除了所有患者中的 6 个人(97%)和 11 个伴有停搏的患者中的 10 个(VASIS IIb)外,血压下降先于心率下降。
在头高位倾斜诱发(预)晕厥中,绝大多数患者(即使根据改良的 VASIS 分类归类为心脏抑制性晕厥的患者),血压下降先于心动过缓发作。此外,随着年龄的增长,心脏抑制性晕厥的频率降低。